The Myth of the Almighty Antibiotic
The Myth of the Almighty Antibiotic
Author: Mark Parkinson RPh: President AFC-CE
Credit Hours 1- Approximate time required: 60 min.
Educational Goal:
To give Adult Foster Care providers the proper perspective about antibiotic therapy.
Educational Objectives:
To dispel myths that has risen around antibiotics
List the types and classes of antibiotic drugs
Define empiric therapy vs definitive therapy vs Prophylaxis Therapy
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.
The Myth of the Almighty Antibiotic
Since the 1940s, Antibiotics have been the wonder drug that has transformed the landscape of modern medicine. Entire diseases have been virtually eradicated from the face of North America. They have worked so well that the myth “The Almighty Antibiotic” has arisen in the public’s mind. For those that believe in the myth, every time a child has an earache, or an elderly mother develops a cough, an antibiotic is demanded by well-meaning caregivers. Belief in the myth is so strong that if antibiotics are prescribed, they are taken only until the symptoms go away, then the leftovers are saved for future illnesses. The truth is, the use of antibiotics is not so clear-cut. Like all therapies, they need to be applied with skill to only those that need it. As with all drugs, antibiotics need to be monitored for effect and side effect, and there is always the risk of allergic reactions developing. In the home, caregivers play a key role in ensuring that antibiotics are utilized appropriately.
Antibiotics (more accurately called antibacterials) are drugs used to treat infections and or prevent bacteria from growing in the first place. They work by either killing outright or inhibiting bacterial growth. Once the growth is slowed, the body’s own immune system can take over and eradicate what’s left of the infection.
Antibiotics were first discovered in 1928 by Dr. Alexander Fleming, who noticed dead zones in a bacterial culture he was growing. He learned that mold had contaminated the culture and had secreted what he called ‘mold juice’ that killed the surrounding bacteria. That discovery led to the development of Penicillin. Since then, hundreds of other antibiotics drugs have been developed. The most commonly used are generally grouped into 10 drug classes:
- Penicillins
- Tetracyclines
- Cephalosporins
- Quinolones
- Lincomycins
- Macrolides
- Sulfonamides
- Glycopeptides
- Aminoglycosides
- Carbapenems

How are antibiotics selected by the doctor?
The primary consideration in antibiotic selection is the effectiveness of the drug at controlling or preventing a bacterial infection. Generally speaking, antibiotics’ effectiveness is determined in three different ways: definitive therapy, empiric therapy, and prophylaxis therapy. Secondary considerations are: the cost of the drug, its side effect profile, its interaction with other drugs or disease states, and the duration of therapy.
Definitive Therapy
In definitive therapy, the responsible microorganism is already known. A pathogenic diagnosis is reached by determining the site of infection, defining the host (e.g., immunocompromised, diabetic, advanced age), and when possible, a microbiological culture diagnosis.
A microbiological culture diagnosis is determined most often in a lab. A sample is grown so that the bacteria can be examined under a microscope. Some bacteria need to be stained with chemicals so that they can be seen and identified easier. The process was first invented by Hans Christian Gram, a Danish bacteriologist. The way the bacteria take the stain helps determine what kind of bacteria they are, generally known as gram positive or gram negative.
Once the bacterium is known, the narrow-spectrum antibiotic can be chosen. Choosing an antibiotic with a narrower scope of effect helps make the therapy more effective. It reduces side effects, the duration of therapy, and its cost. Unfortunately, growing the culture can be difficult and ironically adds additional costs and time. Often the costs are even higher than the benefits gained from the narrower spectrum drug, making definitive therapy prohibitive.
Empiric Therapy
Waiting for a definitive bacterial identification is frequently impractical. Patients are not very patient and usually want therapy now. There are also those who are in such a critical state that waiting would be unethical. Often the doctor can rely on their experience to identify the ‘most likely’ bacterial pathogen. Therapy based on an educated guess is called empiric therapy. In such cases, a broader spectrum antibiotic, which covers a wider range of bacterial possibilities, is chosen.
Prophylaxis Therapy
The third antibiotic therapeutic choice is prophylaxis or applying antibiotics to prevent the ‘possibility’ of an infection. Again, the specific bacterial target is unknown. The antibiotic is chosen based on the ‘most likely’ microorganism that could cause an infection. They are usually shorter, more targeted courses of therapy, sometimes even a single dose. Prophylaxis is usually seen in surgeries, used in dental procedures and to prevent the spread of a known pathogen in a susceptible population.
Problems with antibiotic use
The potency of antibiotics and their ease of administration have spread the use of these drugs throughout the world. In popular culture, there has developed a general anticipation that if you get sick for any reason, you ask for an antibiotic, and things will get better. Antibiotics are asked for even when the patient knows there are no bacteria involved. They think, Let me take them just in case they will help; there will be no harm. The reality is that these drugs are not without side effects, and their popular use has created the potentially dangerous consequence of antibiotic resistance.
Side Effects
It is almost impossible to control where an antibiotic goes once it has been ingested. This creates the potential for unwanted effects. The drug may affect other body processes, interfere with other medications, or kill off the beneficial bacteria that the body relies upon. Each prescription comes with a listing of potential side effects that have occurred in other patients while taking the drug. These side effects may or may not occur in every patient. Even if they do occur, their effect may or may not prove to be significant.
Intestinal Flora Imbalance
In the gut of each person resides a whole world of microbes. It’s a flora of good bacteria (which we rely on), bad bacteria (which could multiply and cause harm), and other microbes like yeasts and molds. We can function normally because this flora is in balance. The good microbes help to keep the bad microbes in check. All antibiotics are designed to eradicate bacteria, even the good bacteria that is helping to maintain the balance in our flora. As a result, every course of antibiotic use has the potential of causing other infections to grow and cause problems. This is a particular concern in patients with compromised immune systems.
Some of the more common antibiotic-caused infections are:
- Clostridium difficile colitis (c-diff colitis)—a bacterial infection which causes diarrhea, fever, and belly cramps
- Vaginal yeast infections in women
- Thrush yeast infections in the mouth and throat (candida albicans)
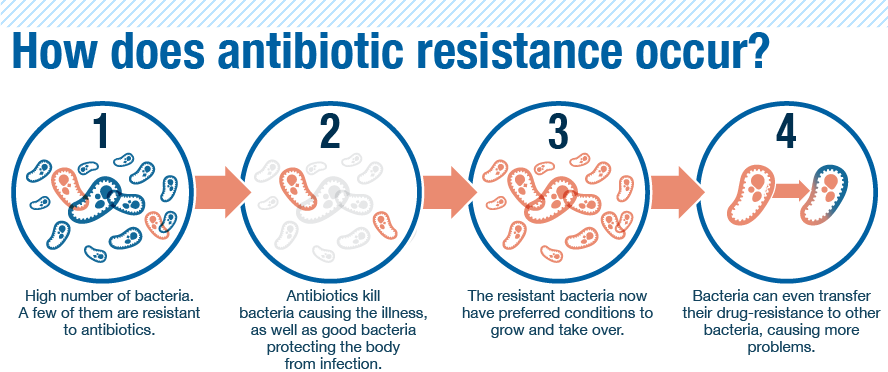
Antibiotic Resistance and Superinfections
By far, the most serious problem in antibiotic use is the emergence of antibiotic resistance, which has caused the rise of superinfections. No two living things are exactly the same. As with all things, there are tiny differences between each bacterium. Some of these variations give the bacteria a survival advantage over others, causing them to grow and reproduce. It’s the natural evolution of the species. The same evolutionary process occurs when antibiotics are taken. The medication does not kill off all of the target bacteria. Those bacteria that have survived and multiplied are now resistant to the antibiotic. If an infection arises from that new resistant strain, other means will have to be used to stop the infection. Eventually, antibiotic-driven evolution creates bacteria that are very hard, if not impossible, to stop. They are commonly called superbugs or superinfections. A superinfection you might have heard about is MRSA (Methicillin-resistant Staphylococcus aureus). It is a very serious infection that has claimed the lives of many victims.
The same resistance evolutionary progression can occur in the cleaning and sterilization processes. In hospitals and other medical facilities where cleaning and sterilization occur regularly, new tougher strains of bacteria have arisen. Infections that are acquired in hospital stays are generally harder to get rid of than those infections acquired in the community at large. Hospital-acquired infections are also called nonsocial infections.
Antibiotic misuse
With appropriate use, followed up by skillful caregiving, antibiotic resistance can be limited. Unfortunately, there are several factors that continue to contribute to the rise of further antibiotic-resistant bacteria:
- Excessive use of prophylactic antibiotics in travelers and medical procedures.
- Inappropriate antibiotic treatment in empiric therapy for illnesses that do not involve bacteria. Commonly, the doctor prescribes the antibiotic ‘just in case’ or because the caregiver or patient demands them.
- Hoarding medication for future use. Patients misuse antibiotics by discontinuing therapy when they start to feel better and saving the drugs. When they get sick again, they take the hoarded medication in hopes that it will save them a trip to the doctor. Often a consequence of this sub-therapeutic dose is that the symptoms will come back within a week or two. This time, the infection is more virulent because it has survived a course of antibiotics.
- The placebo effect of antibiotic medication also occurs because of the mistaken belief in the common myth that antibiotics always help. The belief in the myth is so strong that when the body cures itself, the patient mistakenly attributes the cure to the antibiotics. The reality, though, is, the antibiotics contributed little or did nothing at all.
What is the Caregiver’s role in antibiotics?
 As with all therapies, adult foster care providers play several key roles in antibiotic use in their homes. Caregivers are patient advocates ensuring the residents get the therapies and resources they need. They are also the doctor’s advocate with the patient, ensuring instructions are followed. They are patient monitors, looking for effects and side effects. Finally, they are communicators, educating the resident and informing the doctor about important follow-up information. But besides these obvious roles, the caregiver has several important aspects to be aware of regarding antibiotics and the spread of bacterial infections:
As with all therapies, adult foster care providers play several key roles in antibiotic use in their homes. Caregivers are patient advocates ensuring the residents get the therapies and resources they need. They are also the doctor’s advocate with the patient, ensuring instructions are followed. They are patient monitors, looking for effects and side effects. Finally, they are communicators, educating the resident and informing the doctor about important follow-up information. But besides these obvious roles, the caregiver has several important aspects to be aware of regarding antibiotics and the spread of bacterial infections:
- Watch for the sign of infection after a resident comes from a hospital or nursing home. Common occurrences are upper respiratory infections (coughing, fevers, or runny noses), urinary tract infections (painful urination, deeply-colored or smelly urine, mental confusion), or bloodstream infections (fevers, weakness, general malaise).
- Monitor for the specific side effects listed on the medication information page given with the prescription. Most side effects will go away by themselves when the drugs are discontinued. Notify the doctor if the side effects become troublesome.
- There is always the chance of allergic reactions when taking an antibiotic. True allergic reactions are rashes, hives, itching, fever, swelling, runny nose—and itchy, watery eyes. Even if the reaction is minor, it could get worse with each new dose exposure. All suspected allergic reactions should be reported to the doctor. A few pharmacist tricks to reduce itching is to bath the patient and use a colloidal oatmeal bath preparation or use a sunburn relief first aid numbing spray.
- Anaphylaxis is a rare life-threatening allergic response where the lungs swell up, hampering breathing. Early signs are shortness of breath and wheezing. Call 911 if severe breathing problems occur.
- Upset stomachs, diarrhea, or vomiting are not signs of an allergy but are common reactions to antibiotics. Two pharmacist tricks to reduce the severity of these symptoms are to take the antibiotic with saltine crackers (if food can be taken with the drug). The baking soda in the crackers helps neutralize stomach acid. Also, eating active culture yogurt helps to maintain balance in the intestinal flora.
- When taking care of residents with infections, wash your hands with warm water for at least 20 seconds or use disposable gloves. It may be inconvenient, but it is much better than taking care of a houseful of residents with infections or getting infected yourself.
- It may not be necessary to pressure a prescriber for antibiotics when none is given after a doctor’s visit. Instead, concentrate on requesting symptom-relieving medications to make the resident more comfortable. Acetaminophen (Tylenol) will help with fever and pain but will not help with inflammation symptoms.
Conclusion
The myths of antibiotic use have arisen in popular culture since they were discovered in the 1940s. There is a common belief that there is a pill for every illness and that antibiotics work for every case. Such myths are far from the truth. Patient, doctor, and caregiver actions based on these myths have contributed to the rise in antibiotic resistance and the creation of superinfections. Caregivers play key roles in the proper use of antibiotics and the handling of infections in their residents.
References:
Antibiotics. Wikipedia.com. https://en.wikipedia.org/wiki/Antibiotics
Antibiotics Guide. Drugs.com https://www.drugs.com/article/antibiotics.html
Christian Nordqvist. Antibiotics: All You Need To Know. Medical News Today. Mon 2 January 2017.https://www.medicalnewstoday.com/articles/10278.php
Antibiotics: An overview. Khan Academy. https://www.khanacademy.org/science/health-and-medicine/current-issues-in-health-and-medicine/antibiotics-and-antibiotic-resistance/a/antibiotics-an-overview
Iris Dawn Tabangcora, RN . Antibiotics. Nurse Lanbs.com. Jan 9, 2017.https://nurseslabs.com/antibiotics/
Yvette C. Terrie, BSPharm, RPh. A Patient's Guide to Proper Antibiotic Usage. Pharmacy Times. Dec 1 2014.http://www.pharmacytimes.com/publications/issue/2004/2004-12/2004-12-4835
Exam Portal
click on [Take Exam]
Purchase membership here to unlock Exam Portal.
|
|
|
|
|
*Important*
Registration and login is required to place your name on your CE Certificates and access your certificate history.
Username MUST be how you want your name on your CE Certificate.
| Guest: Purchase Exam |

