Arthritis and Neuropathy Pain
Arthritis and Neuropathy Pain
Author: Mark Parkinson BsPharm: President AFC-CE
Credit Hours 1 - Approximate time required: 60 min.
Educational Goal:
Give suggestions on how to handle complaints of chronic pain caused by arthritis or neuropathy.
Educational Objectives:
- Define what arthritis is.
- Give a brief overview of osteoarthritis and rheumatoid arthritis
- Explain what neuropathic pain is.
- Provide suggestions for the care of the above 3 conditions.
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible
Arthritis and Neuropathy Pain
This CE was requested by one of our subscribers.
Here’s the scene: You get your client up in the morning. She starts complaining of not sleeping well and moaning about her legs or hands hurting. Then she is cranky for the rest of the day, making your life miserable as well. Sound familiar? What is an In-home caregiver to do? Here are a few things I would do. But first, let’s get everyone up to speed on what’s most likely causing the problem: arthritis or neuropathy. Both are tricky to take care of, and caregivers need a good basic understanding of what is going on in the body of their resident in order to manage things effectively.
 Arthritis- What is it?
Arthritis- What is it?
Arthritis literally means joints inflamed. I love how knowing medical terminology makes understanding things that much easier. The inflammation is causing the pain your client is feeling, and the pain is the body’s way of saying to the brain, “Notice me, something is wrong, pay attention”.
So what is going wrong? According to the Arthritis Foundation's website
“Arthritis isn’t a single disease; the term refers to joint pain or joint disease, and there are more than 100 types of arthritis and related conditions. People of all ages, races and sexes live with arthritis, and it is the leading cause of disability in the U.S. It’s most common among women, and although it’s not a disease of aging, some types of arthritis occur in older people more than younger people.”
Types of arthritis
The most common types of arthritis are:

Osteoarthritis- Some call this a wear-and-tear disease, but it’s more than that. Bones in affected joints weaken, and the connective tissue that holds the joint together and covers the ends of the bone deteriorates. Inflammation occurs as a short-term protection against the damage, but chronic inflammation further damages the joint lining. If osteoarthritis continues, eventually much of the joint tissue will be gone. This results in a very loose joint and painful, debilitating bone-on-bone grinding. The body tries to compensate by growing bone spurs around the joint to give the joint some stability. They show up as a lumpy, thickened joint. It is the most common type of arthritis, usually felt in the hands, knees, hips, neck, and lower back. It can happen at any age, but it happens most often as you age. After age 50, it is more common in women than in men.
 Rheumatoid arthritis (RA)- It is an autoimmune disease where the body’s immune system is overactive and attacks some of the tissues in the joints. The disease begins with inflammation in the synovium (joint capsule lining the joint space). Immune cells start to gather in the synovium, leading to swelling and thickening of the joint. These immune cells release further chemicals that damage the bone, ligaments, and tendons, causing the characteristic deformities seen in rheumatoid arthritis. The deformities are painful, limit movements, and cause weakness. The autoimmune response is typically seen first in the small joints of the hands and feet on both sides of the body. The inflammation can spread to other areas of the body. Many people with RA get very tired (fatigue), and some may have a low-grade fever. Anyone can develop RA. It typically develops between the ages of 30 and 60. Children and young adults who have RA usually start to show symptoms between the ages of 16 and 40. Women are three times more likely to develop RA than men.
Rheumatoid arthritis (RA)- It is an autoimmune disease where the body’s immune system is overactive and attacks some of the tissues in the joints. The disease begins with inflammation in the synovium (joint capsule lining the joint space). Immune cells start to gather in the synovium, leading to swelling and thickening of the joint. These immune cells release further chemicals that damage the bone, ligaments, and tendons, causing the characteristic deformities seen in rheumatoid arthritis. The deformities are painful, limit movements, and cause weakness. The autoimmune response is typically seen first in the small joints of the hands and feet on both sides of the body. The inflammation can spread to other areas of the body. Many people with RA get very tired (fatigue), and some may have a low-grade fever. Anyone can develop RA. It typically develops between the ages of 30 and 60. Children and young adults who have RA usually start to show symptoms between the ages of 16 and 40. Women are three times more likely to develop RA than men.
Arthritis is a progressive disease that has no cure. If left untreated, it will only get worse. For the most part, the damage caused by arthritis is irreversible. The goals of therapy are to 1. get a proper diagnosis, 2. slow the progression down, and 3. manage the resulting pain. Early diagnosis is very important in retaining function and managing the pain.
In-home caregivers must pay attention to red flag warnings in the complaints of their residents. You are not diagnosing; you are just suspecting and then asking the right questions of the doctor. If the resident is fatigued, has a low-grade temperature, has swollen knuckles, the pain is felt on the left and right, and the pain or stiffness in the morning lasts longer than 45 minutes to an hour. Start asking questions about rheumatoid arthritis. If the pain is in the fingers, just at particular joints, takes the resident less than 30 minutes to get going in the morning, suspect osteoarthritis. If the pain lasts for more than 6 months, then it's time to see a doctor, regardless of what you suspect. If they already have a diagnosis, then you, as the patient’s advocate, can request the services of a number of specialists who can help you keep your client well and comfortable, and the insurance may pay for the extra care.
Arthritis Specialists Resources
|
Rheumatologist |
RA specialist but often is skilled in all arthritis diseases. |
|
Orthopedist |
Doctor of Osteopathic Medicine (DO). They can also operate as a regular family physician. |
|
Orthopedic Surgeon |
Joint replacement |
|
Pain Specialist |
Excellent resource in managing chronic pain |
|
Chiropractor |
Check the insurance before you go |
|
Podiatrist |
Good resource for all things feet-related |
|
Home Health Nurse |
Great resource for getting doctors to cooperate, and can help get care delegations done |
|
Occupational Therapist |
Helps with activities of daily living. Knows all the latest and greatest tips and tricks |
|
Physical Therapist |
Helps improve movement and function, reduce chronic pain, and prevent future injuries through various treatments and exercises. |
Neuropathic Pain
The other culprit that might be causing discomfort in the extremities of your resident is neuropathic pain. To understand neuropathy, you first have to understand what pain really is. The feeling of pain is just the brain interpreting nerve signals that stress or damage is occurring. If the brain is preoccupied, asleep, or knocked out, the nerve signals are ignored, and there is no pain felt. However, if the nerve is stimulated and it sends signals to the brain, even though there is no tissue damage, pain is still felt. That is what is happening in cases of neuropathic pain. Something is causing the nerves to fire when there is no reason to.
The nerve malfunction can be triggered by multiple factors and can occur anywhere along the nervous system. Even in the brain itself. Common causes are excessive alcohol consumption, diabetes, nerve compression by a tumor, lack of vitamin B-12, trauma, infections like HIV-AIDS, and strokes. Neuropathic pain can be felt as burning, aching, shooting, stabbing or electric shock sensations. It is frequently intense and worsens at night and is often felt in the lower legs. Sensitivity to stimuli is also heightened to the point where a light touch, like feet being covered by sheets in bed or a cool breeze, can cause severe pain. If one of your residents is showing these patterns of behaviors, it might be time to start asking the doctor the right questions so a proper diagnostic exam will be done.
My Suggestions for Caregivers
Pain management in these conditions can be very challenging for in-home caregivers. Your residents are paying you to make them feel content and comfortable. When they aren’t, there is an expectation that you will do something about that. They want you to make the pain go away. Here are a few ideas that can make that happen.
Manage patient expectations
Help the resident get realistic expectations through patient education. Empathetically remind them often of what is actually going wrong and what everyone is doing about it. Also, remind them of what has worked and not worked in the past.
Manage residents' mood
There is a strong relationship between mood and how much pain is felt. Be positive and provide a supportive environment, and the resident will respond. With the doctor's help, actively fight depression. Provide plenty of distractions to divert attention away from negativity.
Get a variety of PRN meds to choose from
Life is variable; some symptoms may show while others fade. Also, the body has a tendency to get used to a pain medication, so it becomes less effective over time. It’s good to have multiple pain therapy tools available to handle changing conditions. Changing up the prn med response can help maintain their effectiveness.
Suggestions to ask the doctor for.
Narcotics (Hydrocodone, Tramadol, Oxycodone). Patients always want to reach for the opioids first. Frequently, that’s all they know. They think that’s the good stuff. Unfortunately that’s not always the case. Narcotics do not take care of inflammation, the root cause of many pain problems. Also, they often are not that effective in managing neuropathic pain. I suggest using them as second-line therapy, what to reach for when other things don’t work.
NSAIDs (Ibuprofen, Naproxen) In my opinion, these are what you should reach for first. By definition, they take care of inflammation. Again not as effective in neuropathic pain.
Acetaminophen (Tylenol) Does not take care of inflammation but does work in the central part of the brain where pain signals are interpreted. An effective alternative when you want to change things up.
Topical meds- lotion, creams, and patches. These are great for changing things up. The massage effect when applying is also therapeutic. If you get approval for self-administration, these agents can give the patient a sense of being in charge of their own therapy. Which is good for their morale.
- Diclofenac (Voltaren) An OTC non-steroidal anti-inflammatory cream that used to be available by prescription only. An excellent alternative for those with sensitive stomachs or medical conditions that limit the use of other NSAIDs.
- Numbing agents- (Salon Paus) Lidocaine is a short-acting numbing agent that inhibits the nerve ending from firing. If it is effective but wears off too soon, you get a long-acting patch.
- Counterirritants- (Bengay, Icy Hot, Asper cream) They work by giving the brain a different sensation to think about, diverting attention away from the pain. Patches are also available
- Capsaicin- Also a counterirritant but in addition has the ability to disrupt certain chemical pathways used to initiate pain signals. This effect is dose-dependent. It has the greatest effect when used often.
- Emu Oil has anti-inflammatory properties

Lotion up the limbs
Applying lotion helps reduce skin irritation nerve stimuli. Massaging the lotion in can also feel really good. It’s an activity of daily living that can double as therapy that does not require a prescription. If you’re doing it a lot though, it is still wise to inform the doctor.
Push for extra help
Don’t be afraid to request the doctor to approve the use of specialists. Contact the resident's insurance to see what is available on their policy. You might be surprised by what a couple of calls can do. If you do get extra help, make sure they go through you as the primary caregiver and major patient advocate.
Reduce the stimuli
Keep the home environment calm and peaceful. Aromas go a long way in calming sensory stimuli. Pay attention to what elements trigger a pain response, then manage them to reduce exposure to pain stimulus.
Plenty of rest, exercise and proper diet
Healthy habits are scientifically proven pain management techniques. Regular exercise and walks are diverting and good for emotional control and improved morale.
Hot and cold packs and heating pads
Alternating hot and cold packs are a proven chronic pain therapy. The cold and heat give the brain something else to think about besides the pain. Heating pads also do this. In addition, ice has a numbing effect and heat stimulates blood flow and promotes healing. This is also a therapy that the patient can control.
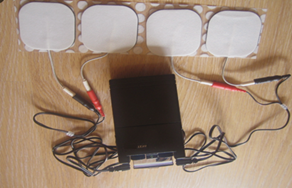 TENS
TENS
Transcutaneous Electrical Nerve Stimulation is an electrical device that sends an electrical current through an area of peripheral tissue. It is also an effective tool in managing pain. In a care home, it will require doctor's approval to use and someone to do a delegation before you can use one. Insurance will require a prescription but some units are cheap enough to just buy one over the internet.
Symptoms Journal
Start keeping a record of symptoms and the circumstances around their showing. It will help you identify triggers, recognize patterns, monitor therapies for effectiveness and side effects, and give the doctor more data to use in determining and managing therapies. It seems like more work, but it can save you a ton of work in the long run.
Conclusion
Chronic pain issues in your residents are also a pain in the neck for you, the primary caregiver. It's difficult and frustrating when you can’t make the problem go away. But there are ways that can help you manage the situation. Don’t be afraid to push the doctor a little. Get plenty of tools in your caregiver tool box, and you will manage things just fine.
As always, Good Luck in your caregiving efforts, Mark Parkinson BsPharm.
References:
- Linda Rath. What Is Arthritis? Arthritis Foundation. Updated June 9, 2022. https://www.arthritis.org/health-wellness/about-arthritis/understanding-arthritis/what-is-arthritis
- NIH National Library of Medicine Medline Plus. Last updated January 8, 2024. https://medlineplus.gov/osteoarthritis.html
- Rheumatoid Arthritis. Cleveland Clinic.Org. Last reviewed on 11/06/2024. https://my.clevelandclinic.org/health/diseases/4924-rheumatoid-arthritis
- Rheumatoid arthritis. Mayo Clinic.Org. April 09, 2025. https://www.arthritis.org/diseases/rheumatoid-arthritis
- Peripheral neuropathy. Mayo Clinic.Org. Sept. 02, 2023. https://www.mayoclinic.org/diseases-conditions/peripheral-neuropathy/diagnosis-treatment/drc-20352067
- Peripheral Neuropathy. Cleveland Clinic.Org. Last reviewed on 10/14/2022 https://my.clevelandclinic.org/health/diseases/14737-peripheral-neuropathy
- Peripheral Neuropathy. National Institutes of Health (NIH).National Institute of Neurological Disorders and Stroke.Last reviewed on August 07, 2024. https://www.ninds.nih.gov/health-information/disorders/peripheral-neuropathy
- Neuropathic Pain. Cleveland Clinic.Org. Last reviewed on 11/13/2023. https://my.clevelandclinic.org/health/diseases/15833-neuropathic-pain
Exam Portal
click on [Take Exam]
Purchase membership here to unlock Exam Portal.
|
|
|
|
|
*Important*
Registration and login is required to place your name on your CE Certificates and access your certificate history.
Username MUST be how you want your name on your CE Certificate.

