Basics of Blood Pressure
Author: Mark Parkinson RPh: President AFC CE
Credit Hours 3.5 - Approximate time required: 210 min.
Educational Goal:
To provide Adult Foster Care providers with information that will help them understand blood pressure and cooperate with hypertension therapy.
Educational Objectives:
- Instruct about the basic concepts that deal with blood pressure.
- Tell how blood pressure is measured
- Discuss Sphygmomanometers and home blood monitoring
- Explain Hypertension
- Explain Hypotension
Procedure:
- Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.

Basics of Blood Pressure
The blood transportation symptom is the body’s super highway. It flows away from the heart in the arteries to the smaller arterials then finally to the tiny capillaries in every part of our body. It transports most of what we need to live. It also carries back from the body’s tissue the waste products leftover from the body’s metabolism. Blood flows from the capillaries to the venules to the veins and then the heart. The beating of the heart is what initially drives the blood through the system. Blood flow is also aided by body movement and controlled by muscles wrapped around the arteries. The flow is shunted to where it is needed by the contraction and relaxation of the muscles around the blood vessels in various parts of the body. The arterial system is kept under pressure. Without blood being under pressure, our body could not get the materials it needs to live. In fact, how much pressure the blood in under is a key indicator of health.
All that is well and good, but I know what some of you are thinking: Why should I even care? What good is this subject to a residential care provider? I’m not planning on performing any surgeries or major medical therapies anytime soon. What good is knowing about blood pressure in my caregiving profession?
I think the key word there is “profession,” as in medical professional. You have to decide whether you just a glorified babysitter and housemaid or something more? I believe that you are something more. Having more patient contact than any other medical profession, I know you have the potential to be one of the most potent members of the health care team. Your potential will only be fulfilled when you start acting like a medical professional. That means that you have to start thinking on a higher level of medical professionalism. That means you got to stop dinkin’ around with the caregiving traditions passed down from your grandmother and replace them with evidence-based proven methods of care.
In the past, hearsay and old wives tales dominated medical practice, but today’s modern medicine is based on evidence and confirmed by measurements. Gone are the days of guessing whether something works - replaced by knowing something works by measuring the vital signs of the patient. Vital signs are the key indicators of a healthy life - heartbeat, body temperature, respiration, oxygen saturation, and blood pressure. If you are going to work on the same level as the rest of the medical team, you have to understand your client’s vital signs. In a practical sense, knowing what’s going on vs. guessing what’s going on makes your job a whole lot easier.
What is blood pressure?
 Blood pressure is the strength of your blood pushing against the sides of your blood vessels in the circulatory system. Your blood’s pressure rises with each heartbeat and falls when your heart relaxes between each beat. How much pressure the blood has at any given point is affected by several factors. It is affected by total blood volume, how thick the blood is, and how much resistance to flow there is. Blood volume and thickness are easy to understand, but resistance to flow needs a little explaining. Unlike a rigid straw for drinking your favorite drink, the blood vessels are very elastic. They easily expand as the blood is pushed along with each heartbeat. The initial pressure caused by the heart is maintained longer because less of the force is lost due to pushing against rigid sides. If there were obstacles in the blood vessels blocking the flow, the pressure would be used up pushing against the blockage. Before the blockage the pressure would increase, behind the blockage the pressure would fall.
Blood pressure is the strength of your blood pushing against the sides of your blood vessels in the circulatory system. Your blood’s pressure rises with each heartbeat and falls when your heart relaxes between each beat. How much pressure the blood has at any given point is affected by several factors. It is affected by total blood volume, how thick the blood is, and how much resistance to flow there is. Blood volume and thickness are easy to understand, but resistance to flow needs a little explaining. Unlike a rigid straw for drinking your favorite drink, the blood vessels are very elastic. They easily expand as the blood is pushed along with each heartbeat. The initial pressure caused by the heart is maintained longer because less of the force is lost due to pushing against rigid sides. If there were obstacles in the blood vessels blocking the flow, the pressure would be used up pushing against the blockage. Before the blockage the pressure would increase, behind the blockage the pressure would fall.
How much pressure is there?
How much pressure there is depends on where and when you measure. There is always some pressure in the circulatory system because of the volume of blood that is maintained by the body. The pressure changes as it moves through the system. It is highest just after a heart beat in the major arteries next to the heart. The pressure is used up as it pushes against smaller and smaller vessels until it reaches the leaky capillaries. As you might guess, the pressure is lowest in the veins of the body.
Pressure is also determined by where and when the blood is needed. As mentioned earlier, a layer of muscle surrounds the arteries that are used to manipulate where the blood flows. This muscle layer plus other factors are used by the body to alter your blood pressure when needed. If the body is too cold, the blood and its heat are maintained in the core of the body. If it’s too hot, it is pushed out to the skin where it can release the excess heat easier. If the body is working hard, the blood pressure is increased to push the blood out to the muscles where it is needed the most. If you get scared or nervous, the blood pressure increases so that you will be ready to “fight or flight.” There is also a 24-hour circadian rhythm, and the body’s blood pressure drops at night when you’re supposed to be sleeping. The bottom line is that blood pressure is extremely variable, going up and down as the result of many factors.
How Is Blood Pressure Measured?
Unless specifically stated otherwise, blood pressure measurements are always taken of the arterial blood supply. Blood pressure readings are given as two numbers (ex. BP 120/78). The numbers are measurements of what happens to blood pressure as the heart is beating. The top number is called the systolic and represents the highest pressure just after the heart beats. The lower number is the diastolic and measures the pressure between beats when the pressure is the lowest. The units of measurement are mm Hg, which stand for millimeters of mercury.
Historically, blood pressure was gauged by how far up a tube it could push a quantity of mercury. Most B/P machines no longer use mercury but the measurement continued.
Blood pressure (BP) can be taken any where there is a pulse, but the numbers change depending on where you take the measurement. The standard placed to take BP readings is just above the crock of the elbow right over the brachial artery. The farther away from this area, the measurements are taken the less standardized the results will be. You might have heard that the farther away from the heart the BP is taken, the less accurate the readings are. It would be better to say the less standardized the measurements are. When taking B/P readings, it is important to report where the blood pressure is taken, for example a wrist or finger blood pressure machine.
Blood Pressure Machines- The Sphygmomanometer
The sphyg what? The word is a combination of Greek and scientific terminology meaning pulse pressure meter. You can call it a blood pressure meter or cuff. There are two types of sphygmomanometers, manual and digital.
Manual- Auscultatory (to hear)
Manual systems are actually two devices used together. One is an inflatable device that is either a manually or an automatic machine pump-filled cuff. The second is a stethoscope for listening to the blood rush through the artery.
The operating principle is easy enough to understand. You wrap the cuff around the arm and place the stethoscope over the artery. Then you inflate the cuff until the atrial blood is cut off. You then gradually release the cuff pressure until you hear through the stethoscope the blood start to gush through the artery with every beat of the heart. That is the systolic or highest blood pressure. You continue to release the cuff pressure until you can’t hear the gushing anymore. That is the point of diastolic blood pressure.
As you can imagine, manual blood pressure machines require skill to use, but they are the most accurate. Unless they have been trained and have regular practice, foster care providers should probably skip using manual devices.
The aneroid (a dial pressure reader) is easier to use but still requires trained skill. The dials also require periodic calibration.
Digital- Oscillometric (electronic calculation)
The easier-to-use but harder-to-understand BP machines are the automatic digital readers. They are basically an electronic pressure sensor. More explanation than that isn’t necessary. There is a complex math formula involved that I know you wouldn’t care about.
Each model has its own instructions, but they all follow the same basic steps as the manual type. Inflate, release the pressure, and read the systolic and diastolic points. Most will also give a read out of the heart rate.
The difference between the various models is how many bells and whistles you want. Ranging from the simplest (and cheapest) hand-inflated cuffs to push-one-button-and-done models. Some of the newer models can be connected to an iPhone so that the BP readings can be sent to the doctor.
The most common models are designed to be used on the arm or wrist, and all are not as accurate as the manual types. They also require calibration from time to time, which also affects accuracy. As an in-home caregiver, getting the most accurate reading is not that big of an issue. You let the doctor worry about getting the most accurate reading. Your biggest concern should be reducing variability by getting the most consistency in your readings.
Caregivers taking home BP measurements 
Regardless of the BP machine caregivers use, the most important factor in my opinion is consistency of use. Have you ever noticed how blood pressure is taken at a doctor’s office? They take blood pressure readings the same way every time. The patient is always sitting in a relaxed position. The same bare arm is most often used etc. The doctor and his staff have been trained to take blood pressures that way to try to control how variable the patient’s blood pressure can be. Just standing up can increase the blood pressure and give a falsely high reading.
In-home caregivers should adopt this same level of professionalism. When you take blood pressure readings, you should do it the same way every time. If there is a change (for example time of day, left arm vs. right), the change should be recorded along with the BP measurement.
Because you can’t always control the situation, caregivers should not be overly concerned with individual readings. Sometimes the pressure readings spike unusually high or low. If you’re concerned over such spikes, wait awhile and take another reading. In my opinion, where Caregivers should concern themselves with patterns that happen over time. If you see a gradual increase (or decrease) or consistently odd read out over the course of several measurements, that is the time to notify the doctor.
What is a normal blood pressure?
I might have given you the impression that BP measurements are all over the place all the time. Going up and down like a ball at a basketball game. Well in the short term, sometimes it can go up and down, but for the most part the body has homeostatic mechanisms that keep thing pretty much the same. When the body is operating normally, the overall average is what is considered normal.
Medical science has not figured out all the control factors that affect blood pressure homeostasis. We do know about the following.
- Baroreceptor reflex- specialized stretch-sensing cells. When blood pressure increases, it makes these cells stretch. They in turn send signals to the brain to decrease the blood pressure.
- Renin-angiotensin system- It increases the blood pressure by constricting the muscles around the blood vessels. It kicks in when there is a drop in blood pressure due to total volume loss.
- Aldosterone- A hormone that helps the kidneys retain salt. Water follows salt so liquid blood volume increases, raising blood pressure.
Our bodies put a lot of effort into keeping the blood’s pressure the same. The brain, nervous system, hormones, muscles, and organs are all involved. All these factors work to bring the body’s blood pressure back to what it thinks is normal. That brings up another point, what’s normal? Describing what is normal in humans is always difficult. Each individual’s reaction to their environment and all the internal control factors of the body make it very complex. The best we can settle for is a range of readings that helps determine what is normal and what is an indicator of ill health. The general consensus is that a normal blood pressure is systolic 90-119 Hgmm and diastolic 60-79 Hgmm. The more fit you are, the lower the numbers become. What we understand as normal also changes with age.
For those readers who take care of children, the blood pressure ranges for children are:
|
Stage
|
Approximate age
|
Systolic
|
Diastolic
|
|
Infants
|
1 to 12 months
|
75–100
|
50–70
|
|
Toddlers and preschoolers
|
1 to 5 years
|
80–110
|
50–80
|
|
School age
|
6 to 12 years
|
85–120
|
50–80
|
|
Adolescents
|
13 to 18 years
|
95–140
|
60–90
|
Source: Pediatric Age Specific UCLA Health System
It’s time for another caregiver reality check. Another “that’s all well and good but what’s in it for me” moment.
Caregiver Moment
As a care provider it is not your job to decide what is normal. That’s the doctor’s job. But the more bloo d pressure readings you take for a patient, the more you will be able to tell what’s an average reading is for that resident. You’re not looking for information that will lead you to diagnose a disease state. You’re looking for red flags that tell you that something needs attention by other medical professionals. If you’re being a medical practitioner yourself and not just a babysitter, you will catch problems sooner and get them resolved quicker. See how that could make your job easier?
d pressure readings you take for a patient, the more you will be able to tell what’s an average reading is for that resident. You’re not looking for information that will lead you to diagnose a disease state. You’re looking for red flags that tell you that something needs attention by other medical professionals. If you’re being a medical practitioner yourself and not just a babysitter, you will catch problems sooner and get them resolved quicker. See how that could make your job easier?
We’re not talking about a lot of extra work or cost either. One $50 automatic-inflate digital model placed on the arm of the residents as they settle in after breakfast, say around 10:00 (when all the morning chores are over) a couple of times a week isn’t much extra work.
When Things Go Wrong
The human body is an amazing thing. The God that made us gave us a wonderful self-regulating creation that can pretty much maintain itself despite all the variables around us. But our bodies are not perfect yet. We’ll leave that process in God’s hand for now. In the here and now, things can go wrong and cause problems. Diseases break things, birth defects handicap us, harmful substances gradually poison us, and bad habits play havoc. We can compensate with drugs, but drugs have side effects that can interfere or they can work too good. Even if we avoid all of the above, eventually things will just wear out. That’s the way we we’re designed. It’s all part of the greater plan for us to eventually move on to bigger and better things.
When things do go wrong, that’s where you come in to help. But how can you help if you don’t know what’s going on.
High Blood Pressure
Chronically high blood pressure in the arteries is called hypertension (HTN). It is a long-term disease state where the homeostatic mechanism of the circulatory system has worn out, is broken, or is being interfered with. The body is built to handle higher pressure in the arteries for short periods of time, so initially we don’t feel a thing. But if the hypertension continues long enough, things start to breakdown. The excessive pressure on artery walls can damage blood vessels as well as organs. The higher the blood pressure and the longer it goes uncontrolled, the greater the damage becomes. Hypertension over time is a major risk factor for hypertensive heart disease, coronary artery disease, stroke, aortic aneurysm, peripheral artery disease, chronic kidney disease, and eye problems. Uncontrolled high blood pressure may also affect the ability to think, remember, and learn.
According to the National Institute for Health (NIH), about one in three adults have high blood pressure. African American adults have the highest rate of almost 44 percent. High blood pressure rates increase with age. The condition is more common in men than women, but after menopause, women’s rates start to increase. Lifestyle has a significant effect on hypertension, resulting in higher rates in lower socioeconomic classes.
Classifying High Blood Pressure
High blood pressure cases have two categories based on the cause of the condition. Primary or essential HTN is the result of a complex interaction of different genetic weaknesses inherent in all of us and the environment that we live in. For example, some individuals are more sensitive to the harmful effects of a high-salt diet than others. Secondary hypertension results from a more identifiable cause. Kidney disease is the most common cause of secondary hypertension (the kidneys are a focal point of blood pressure homeostasis).
Just how high the high blood gets is also an important consideration. The gold standard for the classification of the severity of hypertension cases was set down by the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7).
|
Classification of blood pressure for adults (JNC7)
|
|
Category
|
systolic, mm Hg
|
diastolic, mm Hg
|
|
Normal
|
90–119
|
60–79
|
|
High normal
(Prehypertension)
|
120–139
|
80–89
|
|
Stage 1 hypertension
|
140–159
|
90–99
|
|
Stage 2 hypertension
|
160–179
|
100–109
|
|
Stage 3 hypertension
(Hypertensive emergency)
|
≥180
|
≥110
|
|
Isolated systolic hypertension
|
≥140
|
<90
|
Diagnosis
Traditionally it was recommended that a diagnosis of hypertension be made by the doctor after three separate sphygmomanometer measurements at one-month intervals. The American Heart Association recommended at least three measurements on at least two separate health care visits. There is a problem with that method, a phenomenon call white coat hypertension.
When we get nervous, our blood pressure goes up. Certain people get nervous around doctor offices, so these patients would always give falsely high reading all the time. It wouldn’t matter how many measurements were taken if they were taken in a clinical setting. As a result of these difficulties, greater emphasis has been placed on multiple blood pressure readings taken at home.
Caregiver Moment
Hmm, that will be right down your alley after reading this CE article.
During the diagnosis process the doctor will also look at the patient history and list symptoms he or she discovers. For instance, primary hypertension tends to develop gradually with no apparent cause. Secondary hypertension tends to appear suddenly and cause higher blood pressure. The various conditions that can contribute to secondary hypertension are
- Obstructive sleep apnea
- Kidney problems
- Adrenal gland tumors
- Thyroid problems
- Certain defects in blood vessels you're born with (congenital)
- Certain medications, such as birth control pills, cold remedies, decongestants, over-the-counter pain relievers, and some prescription drugs
- Illegal drugs, such as cocaine and amphetamines
- Alcohol abuse or chronic alcohol use

Risk Factors
The practice of medicine is not only about taking care of problems that have occurred but preventing diseases from happening in the first place. The trick is to identify those who are at most risk and then reduce or eliminate causative factors before high blood pressure occurs.
This is a good place to introduce you to the term prehypertension. According to the JNC7 classification regime above, those with normal but consistently slightly high BP readings are in a warning zone called Pre-hypertension. It is a time where there is no evidence of disease yet but conditions are ripe and may lead to it later on. It is a good indicator that your health is heading in the wrong direction and you should start turning things around by paying attention to the risk factors that contribute to hypertension.
According to the Mayo Clinic, risk factors for developing hypertension are:
- The risk of high blood pressure increases as you age. Through early middle age, or about age 45, high blood pressure is more common in men. Women are more likely to develop high blood pressure after age 65.
- High blood pressure is particularly common among blacks, often developing at an earlier age than it does in whites. Serious complications, such as stroke, heart attack, and kidney failure also are more common in blacks.
- Family history.High blood pressure tends to run in families.
- Being overweight or obese.The more you weigh, the more blood you need to supply oxygen and nutrients to your tissues. As the volume of blood circulated through your blood vessels increases, so does the pressure on your artery walls.
- Not being physically active.People who are inactive tend to have higher heart rates. The higher your heart rate, the harder your heart must work with each contraction and the stronger the force on your arteries. Lack of physical activity also increases the risk of being overweight.
- Using tobacco.Not only does smoking or chewing tobacco immediately raise your blood pressure temporarily, but the chemicals in tobacco can damage the lining of your artery walls. This can cause your arteries to narrow, increasing your blood pressure. Secondhand smoke also can increase your blood pressure.
- Too much salt (sodium) in your diet.Too much sodium in your diet can cause your body to retain fluid, which increases blood pressure.
- Too little potassium in your diet.Potassium helps balance the amount of sodium in your cells. If you don't get enough potassium in your diet or retain enough potassium, you may accumulate too much sodium in your blood.
- Too little vitamin D in your diet.It's uncertain if having too little vitamin D in your diet can lead to high blood pressure. Vitamin D may affect an enzyme produced by your kidneys that affects your blood pressure.
- Drinking too much alcohol.Over time, heavy drinking can damage your heart. Having more than two drinks a day for men and more than one drink a day for women may affect your blood pressure.
- High levels of stress can lead to a temporary increase in blood pressure. If you try to relax by eating more, using tobacco, or drinking alcohol, you may only increase problems with high blood pressure.
- Certain chronic conditions.Certain chronic conditions also may increase your risk of high blood pressure, such as kidney disease, diabetes, and sleep apnea.
Source http://www.mayoclinic.org/diseases-conditions/high-blood-pressure/basics/risk-factors/con-20019580
Treatment
The goal of high blood pressure therapy is to achieve blood pressures below 140/90. Treatment for high blood pressure depends on the cause of the problem. In secondary HTN, the cause is identifiable so that is where the doctor concentrates his efforts. In the more common primary HTN, the cause is unknown and is most likely an accumulation of several factors. In such cases, standard medical practice starts by having the patient make lifestyle changes that bring under control contributing risk factors. If more help is needed, a methodical use of medication is introduced, adding additional medicines until the patient’s blood pressure is under control.
Fortunately in the case of hypertension, small lifestyle changes in many areas can have a cumulative effect, which means several small improvements can make a big difference. For example, in one study, obese teenagers who went on a salt-reduced diet dropped 10 Hgmm in blood pressure after just two weeks. In another example, exercising one hour a day only three times a week can lower blood pressure. It little matters how you reduce your blood pressure. If patients can achieve the goal of less than 140/90, they will realize the long-term benefits.
Caregiver Moment
What that means to care providers is because they control the lifestyles of their residents to a great degree, they can have a huge impact on hypertensive patients. If you regularly monitor B/Ps in the home, you can find out what changes work the best for each resident. It also gives you the benefit of more easily gaining the cooperation of hypertensive residents as you show them the up-to-date progress they are making.

Lifestyle Changes
Lifestyle changes are the first line of therapy in hypertension. The lifestyle changes that care providers can help make that affect high blood pressure are:
- Reduce weight- for overweight residents as little as a five-pound weight loss can start to lower blood pressure.
- Being more active- A 30-minute brisk walk on most days is recommended. In my own care homes, I found that making activity part of the daily routine was the easiest way to start and maintain an exercise regime. I have seen the use of stationary bikes and stepper machines work equally well. Giving the residents active chores to do helps with their health, (as well as relieves their boredom).
- Ban the use of tobacco and alcohol in your homes.
- Decrease salt and increase potassium. An easy-to-implement approach is to replace salt shakers with salt-substitute shakers. You can easily buy products like Mrs. Dash, No-Salt, and Morton Salt Substitute and place them on the table and by the stove. The last two are potassium chloride instead of sodium chloride (salt).
- Stress-free environment- Be aware of the sights, sounds, and feel of the home. Routine is the key to less stress. Periods of relaxing music can go a long way. Another trick is the use of scents in the home. Lavender has a calming effect. Who doesn’t like the smell of cinnamon, even if it is just cinnamon water boiling in a pot on the stove?
- Control contributing conditions like keeping blood sugars under control for diabetics, maintaining blood oxygen levels for those with breathing problems and sleep apnea sufferers, and supporting chronic anxiety suffers.
Food and Eat Healthy
Of all the lifestyle factors that affect blood pressure, eating a good diet is the one thing that is most under the control of in home  care providers. Even though most of you are not licensed dietitians, you can still cook healthy meals.
care providers. Even though most of you are not licensed dietitians, you can still cook healthy meals.
Eating healthy starts with buying healthy. You cook what you purchase, so buy lots of fruits and vegetables, low-fat dairy products, and whole grains. Cooking from scratch is easier to control nutrient values than cooking prepackaged convenient food. You will usually find that cooking from scratch also saves you money.
I think I just heard a collective moan from all the cooks. I know what a big deal food preparation is to an adult foster care home. After planning the menus for over a decade for my homes, I found the secret path to an easier way to cook healthy. It’s all about the recipes. Planning the recipes in advance tells you what to buy, what to have on hand, and how much time it will take and how to cook healthy. Planning the menu through recipes makes everything easier.
Where do you find the right recipes? According to my research, the proven blood-pressure-lowering diets are a Mediterranean-style diet or the DASH diet. Just look them up online, and you’ll find tons of good recipes. DASH stands for Dietary Approaches to Stop Hypertension and was developed by the U.S. National Heart Lung and Blood Institute.
The National Institute of Health (NIH) published an excellent lower-your- blood-pressure guide, which included the following:
The DASH Eating Plan
The DASH eating plan shown below is based on 2,000 calories a day. The number of daily servings in a food group may vary from those listed, depending upon your caloric needs.
|
Food Group
|
Daily Servings
|
Serving Sizes
|
|
Grains and grain
products
|
7–8
|
1 slice bread
1 cup ready-to-eat cereal*
1/2 cup cooked rice, pasta, or cereal
|
|
Vegetables
|
4–5
|
1 cup raw leafy vegetable
1/2 cup cooked vegetable
6 ounces vegetable juice
|
|
Fruits
|
4–5
|
1 medium fruit
1/4 cup dried fruit 1/2 cup fresh, frozen, or canned fruit
6 ounces fruit juice
|
|
Low-fat or fat free
dairy foods
|
2–3
|
8 ounces milk
1 cup yogurt
1 1/2 ounces cheese
|
|
Lean meats, poultry, and fish
|
2 or fewer
|
3 ounces cooked lean meat,
skinless poultry, or fish
|
|
Nuts, seeds, and
dry beans
|
4–5 per week
|
1/3 cup or 1 1/2 ounces nuts
1 tablespoon or 1/2 ounce seeds 1/2 cup cooked dry beans
|
|
Fats and oils†
|
2–3
|
1 teaspoon soft margarine
1 tablespoon low-fat mayonnaise
2 tablespoons light salad dressing
1 teaspoon vegetable oil
|
|
Sweets
|
5 per week
|
1 tablespoon sugar
1 tablespoon jelly or jam
1/2 ounce jelly beans
8 ounces lemonade
|
* Serving sizes vary between 1/2 cup and 1 1/4 cups. Check the product’s nutrition label.
† Fat content changes serving counts for fats and oils: For example, 1 tablespoon of regular salad dressing equals 1 serving, 1 tablespoon of low-fat salad dressing equals 1/2 serving, and 1 tablespoon of fat free salad dressing equals 0 servings.
You can find the whole pamphlet here.
http://www.nhlbi.nih.gov/files/docs/public/heart/hbp_low.pdf
Start your recipe search here: Dash Diet. Keep the beat recipes. https://healthyeating.nhlbi.nih.gov/pdfs/Dinners_Cookbook_508-compliant.pdf

Medication
When lifestyle and diet changes are not enough to reach the target BP rate, clinicians can turn to a wide variety of drugs to help manipulate the circulatory system to lower the patient’s blood pressure. Doctors will usually start off with a lower dose of a single drug (monotherapy) then increase as needed to reach the target BP rate. It is not uncommon to have the patient taking several different medications at the same time (polypharmacy). The drugs will not “cure” the hypertension, just help control contributing factors. If the medication was discontinued, the hypertension would likely return if no other control efforts were made.
Diuretics
Diuretics are commonly called water pills. They work on lowering blood pressure by increasing the amount of salt that is excreted by the kidneys. Water follows salt. If there is too much salt in the blood, then there will be too much water as well. This extra volume is thought to contribute to higher blood pressure. Diuretics help lower the salt content of blood, and the excess water volume follows the salt out in the urine. Diuretics also cause the blood vessels to relax and widen, also contributing to lower blood pressure.
Common examples of diuretics are: Chlorothiazide, Hydrochlorothiazide (HCTZ), Metolazone, Furosemide (Lasix), Amiloride, Spironolactone, and Triamterene.
Special Considerations
- Diuretics should be taken in the morning so that having to go to the bathroom frequently will not be so disruptive to the patient’s lifestyle.
- Some diuretics cause an increase of potassium to be excreted in the urine. The patient might also have to take potassium supplements.
- The patient should be monitored for dehydration.
Beta Blockers
Beta blockers are nerve signal blockers. They work by preventing the norepinephrine and epinephrine (adrenaline) neurotransmitter chemicals from binding to beta receptors on nerves. This prevents the nervous system from telling the muscles around the blood vessels to contract. Wider blood vessels results in lower blood pressure (vasodilation).
Common examples of beta blockers are Acebutolol, Bisoprolol, Propranolol, Atenolol, Labetalol, Carvedilol, and Metoprolol.
Special Considerations
- Unfortunately there are beta receptors throughout the body. Some tell the muscles to constrict while others are related to other effects. Whether these side effects become a problem is very individualistic. Patients should be monitored for dizziness upon standing, breathing problems, blurred vision, constipation, and headaches.
ACE inhibitors
Angiotensin converting enzyme inhibitors or ACE inhibitors lower blood pressure by reducing the activity of a key enzyme in the chemical pathway the body uses to increase blood pressure. Think of as removing a domino in the domino chain the body uses to increase its blood pressure naturally.
Common examples of ACE inhibitors are Benazepril, Captopril, Enalapril, and Lisinopril.
Special Considerations
- Certain populations are sensitive to developing a dry cough that will not go away when on ACE inhibitors.
- Kidney impairment especially when used with an NSAID pain killer and a diuretic.
- They may also increase the pain felt in inflammation.
ARBs
Angiotensin receptor blockers, or ARBs, are drugs that modulate the same chemical systems as the ACE inhibitors, just in another place. They are also commonly referred to as the sartans. They are most often used for ACE inhibitor patients who develop the dry cough side effect.
Common examples of ARBs are Losartan, Candesartan, Valsartan (Diovan) Irbesartan (Avapro), and Telmisartan (Micardis)
Special Considerations
- It is rare, but some ARB patients are still troubled by a dry cough.
- ARB patients should be monitored for muscle cramps, muscle pain, back pain, and insomnia.
Calcium Channel Blockers
Calcium channel blockers or CCBs inhibit calcium from entering cells which is a major “Start or Go” signal for certain cell functions. They lower blood pressure in primarily four ways.
- Vasodilation- Relaxing the muscle layer around the arteries (vascular smooth muscle layer)
- Reduce the force of the contraction in the beating heart. Less force equals lower blood pressure.
- Slow down the heart beat rate.
- Block the kidney from producing a hormone (aldosterone) that is involved with raising the blood pressure.
CCBs are particularly effective against large blood vessel stiffness, one of the common causes of elevated systolic blood pressure in elderly patients.
Common examples of CCBs are Amlodipine (Norvasc), Felodipine, and Nifedipine.
Special Considerations
- Common side effects of CCBs are headache, constipation, rash, nausea, flushing, edema (fluid accumulation in tissues), and drowsiness.
- Caregivers who take care of residents on CCBs should occasionally measure their ankles and lower legs and monitor for a red, hot- looking face (flushing), and unusual tiredness (slow heart rate).
- Monitor heart rate. A normal adult heart rate is 60 – 100 beats per minute. Most digital blood pressure meters also read heart rates.
Alpha 1 Blockers
Alpha 1 blockers, or alpha-adrenergic blocking agents, work similar to the beta blockers just at a different receptor site in the nervous system. Blood pressure lowering is accomplished through vasodilation.
Common examples of Alpha 1 blockers are Doxasosin (Cardura), Terazosin (Hytrin), and Prazosin (Minpress).
Special Considerations
- The body’s homeostatic mechanisms may initially try to counteract the drug’s effect. It may take a while to see the full blood-pressure- lowering effect.
- Alpha 1 Blockers can cause the resident to get dizzy if they stand up too quickly. A way to manage this side effect is to take the medication at night before bed.
- Some drugs in this class can also cause nasal congestion.
There are many other classes of drugs that can lower blood pressure but are not commonly used for that primary purpose. For these medications, lowering blood pressure could be considered a side effect, which the doctor may certainly take advantage of.

Concerns of Hypertension Therapy
There is always the potential to go too far in the drug manipulation of the body’s blood pressure system. There are also the body’s homeostatic mechanisms to contend with and the dynamic effect the environment has on the blood pressure system. Hypertension therapy requires constant monitoring of the patient and dedicated follow through.
Getting Used to Therapy
There is always a transition period in all new medicinal therapies. Caregivers must use patience in the first couple of weeks. Minor problems that occur might go away by themselves as the body gets used to the new drug. If the problems get worse or don’t go away, notify the doctor.
Professionals always have measurements when notifying the doctor. It is not good enough to report: My resident is acting funny. It is much better to report: My resident has an average 138/85 BP taken at 10:00 a.m. for the past two weeks but has experienced a dry cough five days out of the last seven. In my opinion it is always worth the added effort of monitoring and recordkeeping to keep a patient healthy. Healthy residents are always easier to take care of, and professionalism always brings huge rewards in the long run.
Therapy Going Sideways
Side effects are always an issue in drug therapy. Each drug has its own list that caregivers should be familiar with. Common to most (but not all) hypertension medication are the problems of:
- Dizziness upon standing (orthostatic or postural hypotension)
- Electrolyte imbalance (getting sodium, potassium, or calcium messed up)
- Drug working too well (hypotension)
Orthostatic Hypotension
Orthostatic or postural hypotension causes the patient to get dizzy or faint when they sit up or stand. In short, it’s a problem of gravity. When we sit or stand up, gravity pulls our blood toward our toes away from the brain and other vital organs. That lack of blood pressure in the brain even for a short moment is enough to cause problems. Normally our bodies overcome that problem with an automatic response called the baroreceptor reflex or just baroreflex. There are certain nerves that sense a drop in blood pressure in key areas. They send a signal to the brain, which in response keeps the blood pressure up by tightening the muscles around the blood vessels. In essence, the baroreflex squeezes the blood back up to the brain.
Can you see the problem here? Many of the medications affect the nerve signal to the muscle layer around the blood vessels. They may lower the blood pressure but they also may interfere with baroreflex’s ability to squeeze the blood back to the brain when gravity pulls it away. The solution is to get up slowly or raise the body up in stages. If the resident is already unsteady on their feet as is the case of the elderly or infirmed, you have a real concern on your hands. Who cares if the blood pressure is under control if the resident falls and breaks a hip?
Many things can cause dizziness and fainting. To confirm that postural hypotension is possibly the cause of the problem, blood pressure readings are taken after the patient stands. If you get significantly lower readings after standing, it’s time to notify the doctor (for example a loss of 20 Hgmm). From then on caregivers should always be close at hand or even assist the resident when standing or sitting up after lying down for a long time. It’s well worth the extra effort to keep the resident from cracking open their skull on the corner of the table or bed stand.
Electrolyte Imbalance
Electrolytes are the minerals and other chemicals our bodies uses in cell function and to conduct electric signals in the body. A good example of electrolyte function is how the kidneys work to get rid of the waste products in the blood stream. Much of the blood’s content is pumped into the kidney’s tubules, including a lot of the water and its mineral salts. The kidneys then transport the salts back into the blood stream, and the water naturally follows the salts. What’s left is then flushed out in the urine. In addition, the nervous system practically runs on the electoral charge of the sodium and potassium ion charge (Na+, K+).
Can you see the problem here? Many of the drugs used to treat high blood pressure do so by increasing the amount of salt lost in the urine. That’s how water pills work. Also calcium channel blockers alter the way our bodies use calcium, another essential electrolyte. There is always the potential for an electrolyte imbalance.
To prevent electrolyte imbalance, the doctor will blood test on a regular basis. But those blood tests only happen once, maybe twice a year. Caregivers should know the warning signs of electrolyte imbalance for the time in between.
Caregivers should look for the following warning signs:
- Lethargy, confusion, weakness, swelling, seizures, and depression
- Leg cramps and heart palpitations
In-home caregivers will see these symptoms long before any other medical provider, but only if they actively look for them.
Hypotension
Hypotension is the opposite of hypertension or a case of low blood pressure. The body is pretty good at maintaining a constant blood pressure, but there is always a chance in medical therapy that the drugs will work too well and drop the blood pressure to dangerous levels. What BP reading is too low varies by each individual, so caregivers must look for the warning signs and act before any major damage occurs. Generally a BP of 90/60 is considered hypotensive. Your resident will start to look like they are running low on gas because that is exactly what is happening. The blood pressure is too low to carry essential nutrients to the body, especially the brain. Look for lethargy, confusion, irritability, and stuck-in-the mud behavior. Fortunately, this is an easy fix for the doctor, either change the drug or reduce the dose. As a pharmacist, I always thought it was very good news when a patient could reduce the amount of drugs they had to take. What I consider is the most important message in this paragraph is doctors won’t know the dose needs to be lowered if the caregiver doesn’t tell him or her about the hypotension warning signs.
More Information on Hypotension
Very low blood pressure is a dangerous event and often leads to a life- threatening condition called shock. The body’s homeostatic mechanisms work very hard to maintain an adequate blood pressure. It has several interrelated and overlapping compensating systems to keep the blood pressure up. If one fails, then others systems can compensate. One of life’s ironies is the healthier and athletic a person is, the lower his or her blood pressure is. So having lower BP numbers isn’t necessarily an indicator of an inadequate supply of blood pressure. A better indicator is how the body reacts when it starts to run out of essential nutrients the blood pressure supplies.
The brain is particularly sensitive to the lack of nutrients (oxygen and glucose to mention a few). The cardinal signs of hypotension are thus related to brain function, mainly lightheadedness or dizziness. These symptoms can progress to fainting, seizures, and death.
Causes
Low blood pressure is seen is cases of hormonal changes, widening of blood vessels, medicine side effects, anemia, heart problems, or endocrine problems. The most common cause is hypovolemia (low blood volume). I’m not just talking about the blood. An inadequate volume of water could also be the problem. Hypovolemia is caused by excessive bleeding (hemorrhage) and could also be caused by insufficient fluid intake or excessive fluid loss from diarrhea or vomiting. Excessive use of diuretics and heat stroke can also lead to hypovolemia.
Other causes of hypotension are related to troubled cardiac function. Severe congestive heart failure, large myocardial infarction (heart attack), heart valve problems, or extremely low heart rate (bradycardia), often result in hypotension.
Excessive vasodilation (blood vessels are open too wide) is also a source of hypotension. Blood pressure medication can cause vasodilation, also nitrate preparations (nitro pills), sepsis, acidosis, and an excessive use of most inhalation drugs.
Conclusion
 Caregiver Actions in Blood Pressure Issues
Caregiver Actions in Blood Pressure Issues
Wow, we’ve talked a lot about blood pressure, the highs and the lows and a few things in between. We’ve talked about how vital blood pressure is and what efforts modern medicine takes to support the body’s own mechanisms to maintain a healthy blood pressure level.
Most blood pressure issues in care homes will be minor and easily headed off by an alert caregiver. In practical everyday terms, caregivers should look for abnormal behaviors. If there is a concern, the prepared caregiver can confirm any suspicions by taking a blood pressure reading. Remember that one abnormal BP reading could be the machine’s fault. Wait a few minutes and take another one unless it’s obvious that immediate action is required.
And like I always say:
“When in doubt send them out- to the doctor, that is.”
Caregivers should act with medical professionalism, that means less guessing and more facts as seen in measurements. A natural result of this attitude is regular blood pressure measurements taken at home. It will only result in healthier, happier, and easier-to-care for residents.
Good luck in your caregiving efforts.
Mark Parkinson.
References:
1. Description of High Blood Pressure. National Heart Lung and Blood Institute, National Institutes of Health Sep 10 2015 http://www.nhlbi.nih.gov/health/health-topics/topics/hbp
2.High blood pressure (hypertension) Mayo Clinic Patient Care and Health Info. Jul 7 2015 http://www.mayoclinic.org/diseases-conditions/high-blood-pressure/basics/definition/con-20019580
3.High Blood Pressure Symptoms, Causes and Treatments. MedicineNet.com. http://www.medicinenet.com/high_blood_pressure_pictures_slideshow/article.htm
4. John P. Cunha, DO, FACOEP, High Blood Pressure. MedicineNet.com. Feb. 18 2014 http://www.medicinenet.com/high_blood_pressure_hypertension/article.htm
5. High Blood Pressure. Center for Disease Control and Prevention Feb. 19 2015 http://www.cdc.gov/bloodpressure/
6. Self-Measured Blood Pressure Monitoring. Million Hearts, Center for Disease Control and Prevention, U.S. Department of Health and Human Services. Feb.2013 http://millionhearts.hhs.gov/Docs/MH_SMBP.pdf
7. Oscar A. Carretero, MD; Suzanne Oparil, MD. Essential Hypertension Part I: Definition and Etiology. Clinical Cardiology: New Frontiers, American Heart Association Circulation. 2000; 101: 329-335 doi: 10.1161/01.CIR.101.3.329 http://circ.ahajournals.org/content/101/3/329.full
8. Markus MacGill. Blood Pressure: What Is Normal? How To Measure Blood Pressure. Medical News Today. Jul. 9 2015 http://www.medicalnewstoday.com/articles/270644.php
9. Markus MacGill. Hypertension: Causes, Symptoms and Treatments. Medical News Today. Sep 4 2015 http://www.medicalnewstoday.com/articles/150109.php
10. Measuring Your Blood Pressure at Home. Pubmed Health. U.S. National Library of Medicine. Feb. 22 2012 http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0041082/#conssmbp.s3
11. Katrin Uhlig, MD, MS, Ethan M Balk, MD, MPH et all. Self-Measured Blood Pressure Monitoring: Comparative Effectiveness. Effective Health Care Program, National Center for Biotechnology Information Jan 2012 http://www.ncbi.nlm.nih.gov/books/NBK84598/
12. Hypertension. Wikipedia the Free Encyclopedia. Oct. 6 2015 https://en.wikipedia.org/wiki/Hypertension
13. Blood Pressure. Wikipedia the Free Encyclopedia. Oct. 2 2015 https://en.wikipedia.org/wiki/Blood_pressure
14. Sphygmomanometer. Wikipedia the Free Encyclopedia. Aug. 24 2015 https://en.wikipedia.org/wiki/Sphygmomanometer
15. Prehypertension: Are You at Risk? WebMD http://www.webmd.com/hypertension-high-blood-pressure/guide/prehypertension-are-you-at-risk
16. Hypotension. Wikipedia the Free Encyclopedia. Sep. 29 2015 https://en.wikipedia.org/wiki/Hypotension
17. Benjamin Wedro, MD, FACEP, FAAEM . Electrolytes. eMedicine Health. Aug 4 2015 http://www.emedicinehealth.com/electrolytes/article_em.htm
Exam Portal
click on [Take Exam]
Purchase membership here to unlock Exam Portal.
*Important*
Registration and login is required to place your name on your CE Certificates and access your certificate history.
Username MUST be how you want your name on your CE Certificate.

 sound better to say, “I have to take my water pills” rather than “I have to take my urine pills.” Ugh, that does sound unpleasant. It would be more accurate to say, “I have to take my ‘get rid of my extra water by increasing my urine output’ pills.” That’s way too long so most people just say water pills. When communicating with other medical personnel, it is more professional for caregivers to use the correct term of “diuretic.” That’s how I will refer to it for the rest of the article. After all, you are a medical professional.
sound better to say, “I have to take my water pills” rather than “I have to take my urine pills.” Ugh, that does sound unpleasant. It would be more accurate to say, “I have to take my ‘get rid of my extra water by increasing my urine output’ pills.” That’s way too long so most people just say water pills. When communicating with other medical personnel, it is more professional for caregivers to use the correct term of “diuretic.” That’s how I will refer to it for the rest of the article. After all, you are a medical professional.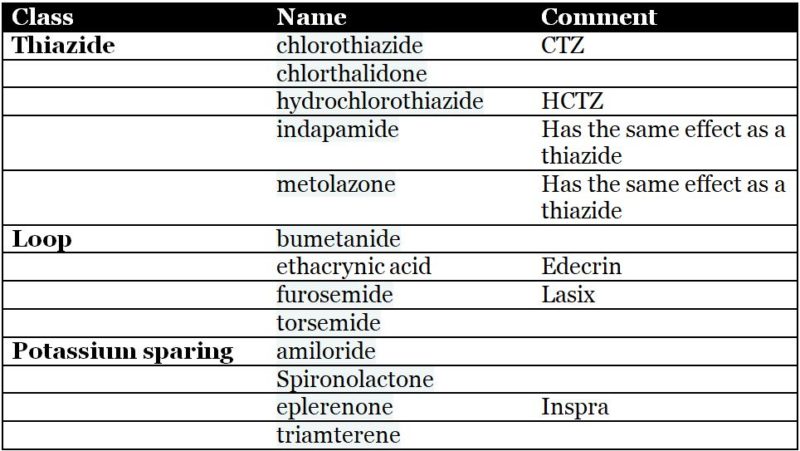


 A Few Special Notes
A Few Special Notes
 Caregiver stress is a common but complex cause of abusive behaviors that is not fully understood. The labor, demands, and conditions on one day might put you on the edge of bursting while other days the same conditions can be managed without stress. It’s hard to know how one day’s reaction differs from another. In my opinion, stress can be defined as an emotional response to environmental conditions that trigger the physical reactions of the body’s flight-or-fight response. Adrenaline and other hormones start to flow, and the body is hyped up, ready to jump at anything. That means that stress occurs not from the burdens we shoulder, but when we feel threatened by those burdens. Again in my opinion, managing stress is more about controlling our reactions to the occurrences swirling around us so that we don’t feel threatened. Of course, that is easier said than done. Here are some ideas that might help.
Caregiver stress is a common but complex cause of abusive behaviors that is not fully understood. The labor, demands, and conditions on one day might put you on the edge of bursting while other days the same conditions can be managed without stress. It’s hard to know how one day’s reaction differs from another. In my opinion, stress can be defined as an emotional response to environmental conditions that trigger the physical reactions of the body’s flight-or-fight response. Adrenaline and other hormones start to flow, and the body is hyped up, ready to jump at anything. That means that stress occurs not from the burdens we shoulder, but when we feel threatened by those burdens. Again in my opinion, managing stress is more about controlling our reactions to the occurrences swirling around us so that we don’t feel threatened. Of course, that is easier said than done. Here are some ideas that might help. susceptible to caregiver burnout. Caregiver burnout is a well-documented source of patient abuse that comes from the physical, emotional, and mental exhaustion of caregiving. You have to deliberately take action to control burnout or burnout will take control of your actions.
susceptible to caregiver burnout. Caregiver burnout is a well-documented source of patient abuse that comes from the physical, emotional, and mental exhaustion of caregiving. You have to deliberately take action to control burnout or burnout will take control of your actions. Spiritual health - Paying attention to spiritual matters really does make you a better caregiver and fights caregiver burnout and all its negative aspects. It reinforces virtuous thoughts, supports the service aspects of caregiving, helps you have a positive attitude, dissuades negative actions, and gives you the social support that is so needed in the isolated world of in-home caregiving. You might think it too difficult, too burdensome to really doing anything “Churchy.” I’m here to tell you it’s doable, and you’ll get more than you give. Here’s a few things that my wife and I did to be “Churchy.”
Spiritual health - Paying attention to spiritual matters really does make you a better caregiver and fights caregiver burnout and all its negative aspects. It reinforces virtuous thoughts, supports the service aspects of caregiving, helps you have a positive attitude, dissuades negative actions, and gives you the social support that is so needed in the isolated world of in-home caregiving. You might think it too difficult, too burdensome to really doing anything “Churchy.” I’m here to tell you it’s doable, and you’ll get more than you give. Here’s a few things that my wife and I did to be “Churchy.”

 There are times when the normal rules of communication go out the window. These are the times that can really stress the caregiver and easily lead to abusive behaviors. By using a few simple techniques, the care provider can successfully navigate through these dangerous waters. Think of these techniques as caregiver tools in your mental equipment box to be pulled out when facing a tough situation.
There are times when the normal rules of communication go out the window. These are the times that can really stress the caregiver and easily lead to abusive behaviors. By using a few simple techniques, the care provider can successfully navigate through these dangerous waters. Think of these techniques as caregiver tools in your mental equipment box to be pulled out when facing a tough situation. It is a sad fact that abuse by caregiver is frequently triggered by resident aggression. Violence and abuse go both ways far too often. It is a normal human behavior to protect oneself from abuse. But unlike other relationships, caregivers don’t get to justify their abusive reactions by saying, “Well he started it, I was just finishing it.” Caregivers have to find ways to control their normal tendencies and maintain control when the resident is abusive to them. Here are a few caregiver tools to add to your mental tool box that might be helpful with an abusive resident.
It is a sad fact that abuse by caregiver is frequently triggered by resident aggression. Violence and abuse go both ways far too often. It is a normal human behavior to protect oneself from abuse. But unlike other relationships, caregivers don’t get to justify their abusive reactions by saying, “Well he started it, I was just finishing it.” Caregivers have to find ways to control their normal tendencies and maintain control when the resident is abusive to them. Here are a few caregiver tools to add to your mental tool box that might be helpful with an abusive resident. If you complain to a doctor and to a lesser extent a home health nurse, most likely you’re going to get a prn prescription that is designed to chemically control a resident’s behavior. In reality, that’s all a doctor can really do to help. Unfortunately, that doesn’t make the problem go away. For most cases, mood-altering drugs are just a bandage. If you as a caregiver rely on these drugs to solve your behavioral problems, you are using a caregiver crutch. They will temporarily help, but they will inhibit you from developing more expert caregiving skills. The more you rely on them solely to solve your behavioral problems, the more your residents turn into zoned-out chemical zombies. At some point, that becomes abuse itself. Speaking as a caregiver and a pharmacist, these drugs are just a tool, not a cure. Add them to the rest of your tool chest and use them with skill, along with the rest of your tools.
If you complain to a doctor and to a lesser extent a home health nurse, most likely you’re going to get a prn prescription that is designed to chemically control a resident’s behavior. In reality, that’s all a doctor can really do to help. Unfortunately, that doesn’t make the problem go away. For most cases, mood-altering drugs are just a bandage. If you as a caregiver rely on these drugs to solve your behavioral problems, you are using a caregiver crutch. They will temporarily help, but they will inhibit you from developing more expert caregiving skills. The more you rely on them solely to solve your behavioral problems, the more your residents turn into zoned-out chemical zombies. At some point, that becomes abuse itself. Speaking as a caregiver and a pharmacist, these drugs are just a tool, not a cure. Add them to the rest of your tool chest and use them with skill, along with the rest of your tools.
















 Stabilize the neck and head if spinal cord injury is suspected. Additional help should be called on to hold the head still while you render emergency care.
Stabilize the neck and head if spinal cord injury is suspected. Additional help should be called on to hold the head still while you render emergency care.





 But when you’re in the caregiving trenches day after day, it becomes easier for caregivers to cross the line. Corners get cut, caregivers get burned out, patients get difficult to manage, and the rights of individuals become forgotten.
But when you’re in the caregiving trenches day after day, it becomes easier for caregivers to cross the line. Corners get cut, caregivers get burned out, patients get difficult to manage, and the rights of individuals become forgotten.
 My Notes:
My Notes:

 Why don’t you take it down and let’s take a gander at it. You have had training from the state on what must be included in each house rules. That training emphasizes the minimum requirements and leaves the rest of the details up to you to figure out. In my opinion, that minimalist training has unintentionally limited the focus of the document, which in turn has limited its usefulness and made it harder to use. So let’s work on some of the details to make it a more functional tool that is also easier to use.
Why don’t you take it down and let’s take a gander at it. You have had training from the state on what must be included in each house rules. That training emphasizes the minimum requirements and leaves the rest of the details up to you to figure out. In my opinion, that minimalist training has unintentionally limited the focus of the document, which in turn has limited its usefulness and made it harder to use. So let’s work on some of the details to make it a more functional tool that is also easier to use.