Credit Hours 2 - Approximate time required: 120 min.
Educational Goal
Teach In-Home care providers how to safely lift and handle resident falls.
Educational Objectives
Inform homeowners of their responsibility in providing training
Present a program of lifting education.
List different types of lifting assist equipment
Cover how to handle resident falls
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.
In-Home Caregiver skill- Proper Lifting
The Blessing and Curse of a Home Care.
Your residents love the laid-back atmosphere of living in a real home. The familiar comforts of home care versus the harsh surrounding of an institutional care setting are a real blessing to them. The curse side of the coin is that home-based care lacks the additional resources found in larger healthcare settings. In a hospital setting if a patient needs to be moved there are machines, devices, and plenty of staff to make the transfer safe for both patient and caregivers. In foster care homes those devices are missing. When a resident needs to be moved or picked up the care provider has to do all the work. If the lift is done improperly the possibility of a career-ending back injury is very real.
Year after year healthcare workers are listed among the professions with the greatest percentage of disabling back injuries. The primary cause of injury is the manually lifting of patients. In nursing homes, it has been reported that injuries to certified nursing assistants (those who actually do the lifting) are three to four times that of registered nurses. The incidents of back injuries among healthcare workers are as high or higher than many professions considered dangerous or hazardous. To make the issue even more serious for care homes. If a CNA gets injured they put them on light duty or hire another CNA. If a foster care owner is injured the business closes. For a foster care home nothing is more serious than that.
Lacking the additional resources and manpower, foster care providers have to mitigate the risk of back injury by working smarter than the problem. Working smarter means acknowledging the risk of injury is real and thinking thru every occurrence of lifting heavy objects. Just because you work in a casual environment doesn’t mean you can be casual about lifting. Care homeowners must make sure that all workers are familiar with the proper techniques of lifting and all care providers need to review those principles on a regular basis.
The rest of this lesson is written as if it is to be used as a training program. I give permission for Care homeowners to copy any portion of this lesson for use in their own business.
In-Home Caregiver Program
Patient Transferring, Lifting, and Falls
Information for Owners - Management Involvement
No program will last for long without the involvement of the boss. Owners of care homes should:
Establish practices and policies for safe patient handling. Owners have to communicate to everyone how to properly and safely lift. You’ll find the easiest way to accomplish this goal is by setting up a program that everyone has to go through.
Elements of such a program are:
communicate the importance of proper techniques.
a training program
a test to demonstrate knowledge gained
follow through.
One idea for training and testing is for the owner or other caregiver to become the patient. Showing and actual hands-on practice, along with reading, is a powerful way to teach.
Supply the proper equipment and resources to accomplish the lifting task. I think I just heard a collective moan from the owners’ wallets. While it is true that a small business must keep expenses down, you’ll find that the proper tool at the proper time does save more money than the tool itself. An inexpensive transfer belt is a lot cheaper than increased worker compensation premiums. More on equipment later. A lot of resources don’t cost any money. These include team lifts. The more bodies that lift, the easier the lifting task is. Owners must establish an environment where workers can ask for and get the assistance they need. If you are getting those types of phone calls, your lifting program is working.
Follow through. It’s one thing to establish a program. It is another to do the program, employee after employee, year after year. A check-off form attached to the employee’s file will help. Make it a habit. Also, keep track of the equipment. Make sure it doesn’t walk off on its own or need repair. Periodically, it is good to ask questions of your employees. Ask them what they need, which tasks are the hardest, should the home be rearranged to make the job easier or safer. This accomplishes several things. Employees can sometimes come up with some pretty good suggestions. It strengthens employee-owner relations. It serves as a reminder of lifting protocols are important. Follow-through is simply a good business practice.
If an injury occurs, reporting it should be one of the first steps. The owner has to create an environment where the employee feels safe reporting an injury. Once informed, the owner has to report it to their worker's compensation insurance program. It’s the law. Failure on either count might lead to denial of a claim, negligence charges, and lawsuits or worse.
Lifting and Transferring Equipment
With medical costs and insurance skyrocketing, large nursing homes and hospital corporations are spending millions on new lifting equipment and implementing no-lift policies. Countries such as Australia have even gone as far as writing the requirements into law. Care homes do not have those resources, but some savvy owners are upgrading their own homes in a more cost-effective way. Make connections with the large health institutions’ equipment managers in your area and you might pick up a good deal on used equipment. Also, keep an eye on second-hand stores where some medical devices can be purchased for pennies on the dollar. You might advertise on the Internet or local newspaper to purchase used equipment.
New patient transfer equipment that is well within the reach of most care home budgets includes:
Transfer or Gait Belts
Traditionally, these were belt-like devices made out of canvas with a metal cinch clasp on one end. It was placed around the hips of the patient, giving caregivers a convenient place to hold on to. While those old belts can still be purchased for less than $5.00 a piece used, they are being replaced by gait belts with a superior design. The new designs are two to three times as wide, made of easy-to-clean synthetic materials, a quick-release plastic clasp, and multiple soft handle loops sticking out. They are easier to use and clean than the older version. They cost a bit more, but new units cost less than $40.00.
Transfer Boards
A transfer board is any material or object that can hold up under the weight of the patient that they can slide on to get from one place to another. Literally, a highly polished board with a good finish will do the trick. Commercial versions are much easier to use for the caregiver and the patient. Transfer boards come in astounding varieties, ranging from simple ones running about $10-20 to extremely versatile or specialized units going for hundreds of dollars.
Swivel Boards or Discs
These devices are placed under the feet of the patient to assist in turning in the pivot-transfer method. They are designed to function even with the heaviest patients. Simple units are fairly cheap. Complex quality units can run up to hundreds of dollars.
Transfer Benches
A transfer bench is a cross between a bath bench and a transfer board. All are designed to be bathtub capable. The simplest is just bath benches that are long enough to extend over the bathtub side wall. Used versions can be picked up inexpensively. More advanced versions come complete with swivel chairs mounted on rollers. They make bathing your residents very easy and virtually fall-free. They run up to $500, depending on how many features you want. Good units can be purchased for around $200- $400 each.
Power Lifts
Power lifts are any powered device that aids in a patient's standing or transferring. These are the most expensive, with some devices running thousands of dollars. The most common versions in care homes are power lift recliner chairs that residents bring with them from home. Make arrangements to purchase used chairs when a client moves on. Or better yet ask the family member to donate the chair.
Stand-Assist Devices
Stand–assist devices are basically, handles that the patient holds on to while they stand. The patient uses them to pull themselves up. The model can be free-standing or fixed to a bed, or chair. There is even a version that attaches to the top of a car door which makes it easier to get in and out of the car. These are simple devices and most can be purchased for $100 or less.
Insurance Coverage
Depending on the patient’s diagnosis, some devices are covered by insurance. A durable medical device salesman can assist you with the particulars of the paperwork. A prescription will likely be needed. It would be to your benefit to learn about the insurance process so you can utilize the coverage in similar future circumstances.
Care Provider Training Program
Overview
Every year, thousands of healthcare workers go to work to help their patients only to have a lifting injury and become a patient themselves. It is ironic that the act of assisting the patient, if not properly done, may cause harm to that very patient. To help keep you and your charges from unwanted injury, the following program was developed.
A well-meaning caregiver about to hurt her back
Awareness
In-home caregiving may seem like an easy job, but at times it can be quite physically demanding. The caregiver must take the responsibility to always be aware of what is required of them and accomplish those tasks safely. Do not fall into the trap of doing things the quick and sloppy way. Such thinking has led to many patient injuries, caregiver back surgeries, and lives full of pain.
If an injury does occur, report it immediately. A stitch in time really does save nine. No one wants to see you injured or work while you are in pain. Call the management at any time when there is a need. Help will always be there for you.
Limitations
Remember that when you work with the elderly or bedridden, inactivity and osteoporosis rob the bones of their strength and make them brittle. Arthritis can result in sore and stiff joints, making regular movements difficult. It’s easy to get dizzy if you get up too fast. Some patients have injuries that make one side weaker than the other. Always try to compensate for the weak side.
Before the Lift
Think about what you are doing. Figure out the proper lifting technique for the task at hand. Utilize the proper equipment, clear the area or path of hazards, and get help if you need it. Gather the items you need before the lift or transfer. Never leave an “at-risk” person alone in a precarious position.
A Special Note: Get Help
You are not in this alone, and you are not superhuman. If the lifting is too heavy, get help, either from the proper equipment available or the assistance of someone else. Many hands always make lifting easier and safer.
Know Your Patients
Everyone has varying capabilities and weaknesses. If you are new to the job, make it a priority to learn what disabilities your charges have. Don’t be surprised in the middle of a lift that a patient can’t do this or that function. Always be aware that patients can have bad days that reduce their capacities.
Proper Body Mechanics
Every lifting job is different, but there are common elements to all proper lifts or patient transfers
Face the person or object and establish a solid base of support. Place your feet shoulder length apart on the solid, slip-free ground.
Keep your back straight.
Bend at the knees and not the lower back as much as possible.
Hold the object as close to you as possible.
Tighten your stomach muscles when lifting.
Lift as much as you can with your legs.
Never twist when you lift. Make adjustments with your footing instead.
Push rather than pull when you can.
Maintain good communication in team lifts.
Lift with smooth efforts, with no sudden jerking.
Patients are not the only heavy things that you might be required to lift. A 25-pound bag of potatoes, flipping a mattress, or moving furniture around can overstrain the back if improper body mechanics are used.
Patient Transfers
Moving a patient from one place to another is an essential required skill for any caregiver. But awkward positions, tight, in-home spaces, and unpredictable patient movements can make transferring a patient a dangerous task. Over the years, techniques have been developed that will enable you to move the patient easily and safely.
Rolling a Patient in Bed
Ensure that there is enough room to roll the patient in the direction that is needed.
Have the patient bend the opposite knee in the direction you want to roll.
Cross the opposite arm you want to go and have the patient reach in that direction
Place your hands on the shoulder and hip area and gently push until the roll is complete.
Setting the Patient on the Edge of the Bed From a Reclining Position
Bring the patient to the edge of the bed. This may take leveraging from top to bottom a little at a time. Avoid pulling heavy patients all at once.
Dangle both feet over the edge of the bed.
Put one arm under the patient’s shoulders and one arm over the hip, slightly lower down the leg.
Start by pulling the lower half of the body over the edge of the bed and then utilizing the natural pull of gravity lift from the shoulders until the patient is upright.
Note: if the patient is so large that it puts you in an awkward position, you might have to divide the task into two steps. Legs first, then lift the shoulders.
Transferring From Sitting to Sitting. Pivot Transfer
Secure the transfer destination. If it is a wheelchair. place it against the bed. Lock the wheels. Remove or swing away the footrests. Remove the arm of the chair that is against the bed, if required.
Bring the patient to the edge of the thing they are sitting on (bed, chair, or car seat).
Utilize a transfer belt, if one is available.
Place your foot in front of the patient’s toes to prevent slipping.
Bend at your knees and reach around and grab the patient’s belt.
Tell the patient you’re about to lift and count to three. If there is some difficulty, you can start a forward rocking motion on each count, one, two, and lift on three.
Have the patient push off with their hands or place their hands on your shoulders or upper arms, never around your neck.
Lift straight up utilizing the natural pull of your weight and lift from your legs. Tighten your stomach muscles to help take the strain off your lower back. Never lift from your lower back muscles.
Once the patient is standing and while you are still holding the belt, turn the entire body by taking small steps with your feet. Do not twist from the waist.
Gently support the downward movement of the body by bending your legs and keeping your back straight until the patient is safely seated. Keep the patient in your center of gravity by placing your feet on the outside of the patient’s feet and your knees on the outside of the patient’s knees.
Note: Position the destination chair on the strong side of the patient. Provide verbal cues for example, “turn, turn, OK, sit.” Positioning the receiving wheelchair at a slight 30-degree angle creates a bigger receiving “target” for the patient.
Repositioning the Patient in a Chair
Have the patient lean forward with their shoulders toward their knees.
Place yourself in front of the patient with knees against the knees of the patient.
Bend at your knees and grab hold of the patient’s belt (or transfer belt if it is needed).
On the count of three, roll your feet onto your toes and push with your knees against the patient’s knees, utilizing your own natural leverage to lift the patient’s bottom off the cushion.
Gently slide the patient forward into the desired position. Don’t lift the patient.
Sliding Board transfer
A transfer board is any sturdy board that is placed as a “bridge” between two positions and the patient slides to their destination.
Place the patient at the edge of the place they are sitting on. Lean the patient away from their destination.
Place one end of the board under the elevated hip. Be careful not to pinch the skin. Place the other end at the destination securely.
Have the patient “scoot” along the board with your guidance so they do not lose their balance and fall. Let the patient do the work or if necessary use several abbreviated pivot transfers.
Note: Utilize gravity by making the destination lower than the starting position if you can. Have the patient take advantage of any secure handholds that are available. For difficult transfers like from a small car, an intermediate destination might be of use, utilizing two transfer boards.
Special Notes for Transferring the Patient to a Car
Make sure the car seat is moved back as far as it can go. Recline the back of the seat slightly to provide more room. After the patient is in, you can straighten the seat into a more comfortable position. Roll the window down so that the car door can become a handhold.
What To Do in Falls
A patient falling is always a major concern. Unfortunately, it is almost inevitable with In Home care that a patient will end up on the floor. Keep your ears tuned in. It is most likely you will hear a fall before you see one. Prompt action is required. Always inspect the area and the patient before taking any action.
Lifting a patient from the floor is particularly dangerous for the patient and the caregiver. If the lift is not done right, the patient can suffer further injury and the caregiver can end up injured, too.
First: Prevent the Fall in the First Place
As you walk with the patient, find the center of balance and place your hand there. For most, it is the lower back, conveniently close to the belt line. Grab on the belt, if there is one. If you need to, apply a transfer belt. As you walk, feel for unusual movement and give balance when needed to keep the patient on their feet.
Many falls happen when the patient tries to get up to fast. Do not pull the patient up from a relaxed position all at once. Set them up and tell them to get ready to stand up. Make sure they scoot their bottom to the edge, straighten up, firmly place their feet, and get their balance ready.
Transfer boards are handy when going from sitting to sitting positions or standing to a difficult sitting place, for example, getting into a car or bathtub. Place a stool or chair outside the car or tub and place the transfer board between them. Have the patient sit on the transfer board and slide the patient to their destination.
Second: During the Fall
Usually, you can keep a patient upright by helping to maintain balance, but there are times when that isn’t going to be adequate. Sometimes the patient is going down no matter what you do. Don’t let them take you down with them or jerk your back out of place as you try to assist them.
If the patient is falling, do not try to stop it. Control the fall instead.
Steer the fall to a safe place.
Slow the speed of the fall down from YOUR center of gravity, bending properly as you go down. A safe way is to drop your center of gravity a little slower than the patient.
Protect the patient’s head.
Let the patient slide down your leg to the floor. Bend at the hips and knees as you lower them.
Third: After the fall
If you were not present when the patient fell, first be sure the area is safe for you to go into. For example, be aware of electrical wires and broken glass hazards. When a patient falls, most will want to get up right away. Don’t let them until you have made an injury assessment.
Injury Assessment
Call the care home owner and 911 as per company policy when the patient has lost consciousness, has uncontrolled bleeding, stopped breathing, if the pupils are dilated inappropriately for the room lighting or if one pupil is larger than the other, or any other life-threatening circumstance. If you feel overwhelmed, call the care home owner.
Check for a sign of a fracture. The patient will report pain, tenderness, or hearing a pop or snap. You might notice swelling or bruising.
Hip fractures are of particular concern and are noticed by one leg being shorter than the other, there is an unusual angle to the leg, or the patient feels or hears a “crackling” when they move or they are unable to move. If a hip fracture is suspected, DO NOT move the patient. Make them comfortable and get help immediately, then keep them warm with a blanket.
Assess for signs of confusion or altered speech. Questions you can ask are: What year is it? Do you know where you are? Which room is yours? What were you trying to do before you fell?
Check for cuts and bleeding from head to toe. Skin tears look very severe but they are usually not life-threatening. Head cuts have a tendency to bleed a lot, even minor ones.
If you suspect a head, neck, or spinal injury, DO NOT move the patient. Get help immediately.
When calling 911, be calm and communicate clearly. Note any pertinent details. It is better to give too much information than not enough. Always call the care home owner, too.
If There Are No Injuries
If there are no injuries that you can see, help the patient get up in stages. There are several reasons for doing this. Unnoticed injuries will present themselves sooner and you can abort the attempt easier and safer. It saves you from lifting the dead weight of the patient. It’s also good for bruised egos and embarrassed patients to do the work themselves. It makes them feel less of an invalid.
Stages from the floor
Turn the patient over until they are on their knees, using proper patient roll technique.
If there is an object close by like a chair or bed, guide them in crawling to the object.
Have them lift one knee up.
Lift the patient to an upright position, utilizing proper body mechanics. If needed, have a chair nearby and lift them to the seat first then stand them up. Do all these steps slowly with plenty of time for patient orientation in between steps.
Note: patient transfer belts make the operation easy for you and safer for the patient.
Conclusion
Do your patient, yourself, and your back a favor and be prepared before you lift or assist in transferring a patient. Know proper lifting techniques before you lift, and think through every lift before you act. Get the necessary equipment or help, use proper body lifting mechanics, communicate clearly, and lift with safety in mind. Remember, furniture and heavy supplies can be just as damaging to you as an improper patient lift. Helping others shouldn’t result in injuring yourself or the patient. Remember, you won’t be helping anyone if you find yourself on the wrong side of back surgery.
As always Good Luck in your caregiving efforts.
Mark Parkinson BsPharm.
PS:
Good care providers are in short supply nowadays. Take good care of yourself. You are way too valuable a resource to your community and those who depend on you.
References:
Richard F Edlich et al. Devastating injuries in healthcare workers: description of the crisis and legislative solution to the epidemic of back injury from patient lifting. Journal of Long-Term Effects of Medical Implants. 2005;15(2):225-41. doi: 10.1615
Credit Hours 4 - Approximate time required: 360 min.
Educational Goal
Provide In-Home caregivers a guide on becoming familiar with heart disease.
Educational Objectives
Describe the Anatomy of the heart
Review the Physiology of the Cardiovascular system
Familiarize the reader with the pathophysiology of the most common occurs of the heart
Explain the major risk factors for developing heart-related problems
Tell how to work with doctors
List Coronary system tests
Provide guidance for Caregivers on how to manage heart disease factors and medications.
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.
A Caregivers Guide to Heart Disease
Arguably one of the most important organs in the body is the heart. It is a remarkable organ that is responsible for pumping life-sustaining blood throughout the body. It is constantly working 24 hours a day, seven days a week. The more you work it, the stronger and more efficient it becomes. It works so well and so consistently that we take it for granted until something goes wrong. When things go wrong for the heart, things go wrong for the entire body.
The leading cause of death since 1950 is heart disease, a collection of pathological conditions affecting the heart and circulatory system of the body. Altogether they account for approximately 30% of deaths in the US. That figure represents one person passing away from problems related to the heart every 34 seconds. Heart disease costs the United States about $229 billion each year. That cost includes health care services, medicines, and the loss of productivity due to illness and death.
There are multiple risk factors for developing heart disease, ranging from genetics to lifestyle choices. Literally everyone is either born with or can make bad lifestyle choices that can potentially lead to heart problems. Heart disease is preventable and if it does occur it is manageable. Unfortunately, once it has developed the risk of worsening conditions will always be present.
The heart is remarkably resilient. Normally it takes care of itself. If heart disease does develop the patient can still lead a normal life if healthy lifestyle choices are made and therapy adhered to. In-home caregivers are in an excellent position to ensure that proper lifestyles are maintained, and medical orders are followed correctly. Caregivers can be more effective in these roles if they have a greater understanding of the heart and its pathological conditions. This course is designed to start you on the journey of achieving that goal.
Anatomy of the Heart
The heart and its circulatory system are too much material to cover. You’d fall asleep by the time I’d have finished covering it. I’ll only cover the material I think that you need that will help you manage your residents well and communicate effectively with other medical professionals. Also, I want to make things a bit more entertaining so I am going to slip in a video or two. You play the video by clicking on the start arrow. If you want the image bigger, click on the full-screen box icon in the lower right corner. When you are done watching, click on the same icon to shrink it down to size. There will be quiz questions covering the video materials. Sorry about the ads if they come up on your computer, it’s what makes the videos free for me to use.
That was the big picture. Now let’s take a look at the little details. The cardiovascular tissue is mostly made up of connective tissue, nerves, and muscle. Around the blood vessels is special muscle tissue called smooth muscle. They are designed to operate automatically in response to signals from the attached nerves. They tighten around the blood vessels to narrow the passage and increase blood pressure or loosen up to drop the pressure. For example, when you stand the blood is pulled away from the brain by gravity. The smooth muscle compensates for gravity’s pull by tightening up around blood vessels. The extra pressure keeps more blood in the brain, so we don’t pass out. The blood vessels provide a pathway for the blood to move around the body. The smaller the passageway becomes the leakier it gets. This allows nutrients, fluids, and such to pass out to the tissues where it’s needed. Waste products are moved into the veins and transported to the organs that take care of the unwanted material. The first two factors will be important when we talk about the pathophysiology of the heart and the medication used to treat it.
The walls of the heart have three layers. The innermost layer is the endocardium. It covers the heart chambers and heart valves and connects to the tissue lining of the blood vessels. The outermost layer is called the epicardium which forms part of the pericardial sac that surrounds, protects, and lubricates the heart. The bulk of the heart wall is made up of the middle layer called the myocardium. It contains the specialized cardiac muscle cells that do most of the work of pumping the blood around. They are different than the other muscle tissues of the body in that they are 1. More connected physically and electrically to each other. This allows the heart tissue cells to work as one. 2. Have more intracellular structures that produce energy, allowing them to work all the time. Under normal conditions and given enough supplies they will work continuously without becoming fatigued. This will become important when we talk about heart attacks.
The last heart tissue that we need to talk about is the pacemaker cells. They are specialized nerve cells that are set up to fire automatically in a coordinated fashion on a set schedule. There are two bundles of them located in the right atrial chamber of the heart. The first to fire is the bundle called the sinoatrial node (SA node). It makes the atrial chamber muscle contract as one, pushing the blood into the ventral chambers. There is a small delay then the electrical signal reaches the atrioventricular node (AV node), and they fire. This signal makes the ventral muscle contract as one and they push the blood out and away from the heart. This coordination of nerve firing is essential for the regular rhythms of the heartbeat. The regular rhythm of contraction is referred to as sinus rhythm because the electrical impulses are generated by the sinus node.
Pathophysiology of the Heart
Permanent damage and the new normal
The heart and the cardiovascular system are an extremely dynamic and robust system. They can adjust easily to the changing demands of the body and quickly repair any damage that occurs. But there are limits to which the system can cope. Exceed these limits and permanent damage starts to occur. At first, you may not even notice the changes the damage is creating. Eventually, though there is so much permanent damage that it becomes debilitating and even life-threatening. Medical interventions and surgery can help compensate, but the cardiovascular system will never return to its normal functioning. In layman’s terms once you have heart disease you will always have it. You will be forced to adjust your lifestyle or face further heart troubles down the road. Helping the patient adapt to the new “normal” is what In-Home caregivers should be focused on. More about that later.
Types of Heart Disease
Heart disease is a general all-inclusive term that includes a range of conditions that results in heart problems. It's also called cardiovascular disease, which means heart and blood vessel disease.
Heart disease includes:
Congenital Heart Disease (CHC)
Coronary artery disease
Irregular heartbeats (arrhythmias)
Heart valve disease
Diseases of the heart muscle (cardiomyopathy)
Heart Failure
Congenital Heart Disease
Congenital Heart Disease is also a general term for patients who have one or more defects in the heart’s structure since birth. Its symptoms range from mild to life-threatening and can alter the way blood flows through the heart. Problems resulting from these defects can appear at the moment of birth or may only manifest themselves later on in life. Common congenital heart disease symptoms in adults include:
Irregular heart rhythms (arrhythmias)
Blue skin, lips, and fingernails (cyanosis)
Shortness of breath
Feeling tired very quickly with activity
Swelling of body tissue or organs (edema)
For some people, the signs or symptoms of congenital heart disease aren't noticed until adulthood. It is also possible that symptoms may return years after a congenital heart defect is treated. Once diagnosed, patients will require at the very least regular doctor checkups. Most likely though, lifelong medication use or even surgery will be needed.
Coronary Heart Disease
Coronary Heart Disease also known as Coronary Artery Disease (CAD), is the most common form of heart disease. CAD occurs when the walls of coronary arteries supplying the heart become hardened and narrowed. This reduces the hearts’ ability to work hard and makes it easier to have a heart attack or stroke. It almost always occurs because of a buildup of fatty plaque on the walls of the arteries.
To understand why the plaque starts to build up you must first know that this is a long slow process that may take years to develop. First, the arterial wall is damaged because of things like prolonged high blood pressure. Inflammation occurs as part of the repair process. Too much exposure to inflammation can cause greater damage to the inner arterial wall. This creates a place where fatty material like lipids and cholesterol can stick and collect. If the harmful condition persists the plaque continues to build until the passageway is narrowed.
A person with plaque buildup will mostly not feel any adverse effects, but…. Plaque is not a durable material. Bits of plaque can break off and lodge downstream in narrower arteries. The plaque can also burst, accidentally setting off the clotting process inside the artery. The result is a blocked flow of vital nutrients like oxygen and the rapid build-up of toxic waste material. Cells will start to die. If it happens in the brain, you have a stroke. If it happens in the heart, you have a heart attack.
The following video is for the advanced reader. There will not be any test questions on it. For those who brave it anyway, you will see it is an excellent visual explanation of the clotting cascade of a heart attack.
The signs and symptoms of CAD depend on where the arteries are narrowed. For example- pain, numbness, weakness, or coldness in the legs or arms may be the result of the narrowing of the arteries in the limbs.
If a coronary artery is totally blocked, every cardiac cell downstream is going to be in a world of hurt. Kill off enough cardio muscle and the heart will stop functioning. You know what suddenly follows after that.
The outward signs of a heart attack are:
Chest pain or discomfort. Most heart attacks involve discomfort in the center or left side of the chest. It lasts for more than a few minutes or goes away and then comes back. The discomfort can feel like uncomfortable pressure, squeezing, fullness, or pain.
Feeling weak, light-headed, or faint. You may also break out into a cold sweat.
Pain or discomfort in the jaw, neck, or back.
Pain or discomfort in one or both arms or shoulders.
Shortness of breath. This often comes along with chest discomfort, but the shortness of breath also can happen before chest discomfort.
If the coronary artery is only partially blocked, the heart can continue to beat. But there will still be problems. Men and women may experience different coronary artery disease symptoms. Studies have shown men are more likely to have chest pain. While women are more likely to have other symptoms along with chest discomfort, like shortness of breath, nausea, and extreme fatigue.
Angina
Angina is a type of chest pain caused by a reduced flow of blood in the heart. Angina sufferers describe it as a feeling of squeezing, pressure, heaviness, tightness, or pain in the chest. It may also feel like a heavy weight lying on the chest.
Angina is not a heart attack, but it is often a precursor to it. There are different types depending on the cause and whether rest or medication relieves symptoms. Being familiar with the different types gives caregivers important clues as to how to react to the situation and what to report to the doctor or emergency medical personnel.
Types of Anginas
Stable angina.
The most common form of angina. It usually happens during activity (exertion) and goes away with rest or angina medication. For example, pain that comes on when walking uphill or in cold weather. Stable angina pain is predictable and usually similar to previous episodes of chest pain. The chest pain typically lasts a short time, perhaps five minutes or less. Record events and look for long term patterns of frequency or severity
Unstable angina
(a medical emergency)
Unstable angina is unpredictable and occurs at rest. Or the angina pain is worsening and occurs with less physical effort. It's typically severe and lasts longer than stable angina, maybe 20 minutes or longer. The pain doesn't go away with rest or the usual angina medications. If the blood flow doesn't improve, the heart is starved of oxygen and a heart attack occurs. Unstable angina is dangerous and requires emergency treatment. Call 911
Variant angina (Prinzmetal angina)
It's caused by a spasm in the heart's arteries that temporarily reduces blood flow not caused by CAD. Severe chest pain is the main symptom of variant angina. It most often occurs in cycles, typically at rest and overnight. The pain may be relieved by angina medication.
Refractory angina
Angina episodes are frequent despite a combination of medications and lifestyle changes. Standing orders from the doctor may be required
Arrhythmias are any sequence of nerve cells firing that causes a heart rhythm that is not a normal sinus rhythm. It can be a single extra beat causing a palpitation to a quick uncoordinated firing causing a heart chamber to quiver.
Some related terms you might have heard are;
Bradycardia- Slow heartbeat
Tachycardia- Fast heartbeat
Fibrillation- Irregular heartbeats, often very fast
Atrial Flutter- Regular fast contraction of the atria heart chambers
Heart Block- The electrical signal that controls the heartbeat is partially or completely blocked.
Here is a quick video on arrhythmias
Arrhythmias can be continuous or intermittent. Sporadic irregularities can be difficult for the doctor to diagnose. They usually occur when the doctor is not listening or performing a medical recording of heartbeats. Both typically last for just a few seconds. A 30-day heart monitor may be worn by the patient. It will give the doctor a greater source of data that will help in assigning a diagnosis.
The factors that can contribute to arrhythmias include heart disease, high blood pressure, diabetes, smoking, heavy alcohol use, an electrolyte imbalance, drug abuse, and stress. Certain medications, herbs, and dietary supplements can also cause or aggravate the condition.
Irregular heartbeats can lead to irregular blood flow. Irregular blood flow increases the chance of unwanted blood clots that can cause significant harm. It is not uncommon for blood thinners to be prescribed in such cases as a preventative measure.
Arrhythmias also may or may not be felt by the patient. Hear again intermittent occurrences can cause a lot of fear and anxiety in the patient. In-Home caregivers can be of calming assistance by
Keeping good records of occurrences and passing the info on to the doctor.
Advocate for the need for a cardiac specialist.
Assist with any specialized equipment used.
Monitoring for irregularities
Providing a safe environment that lessens the risks of injury from fainting
Real World example. Recently my mother-in-law was plagued by fainting spells. Her regular doctor was at a loss, blaming it on a side effect of her medication. The condition worsened and she was hospitalized. She even fainted while in the hospital. Finally, I moved her into my home and got her to see a cardiologist. He placed a 30-day monitor on her that was connected remotely to the internet. He was able to see the data from his office. After the thirty days were over, he was able to notice an arrhythmia that was occurring only 3% of the time. He called it a sick sinus syndrome caused by her natural pacemaker cells not firing or being blocked. He told us that it was a common condition resulting from the aging process. He surgically implanted an artificial pacemaker and said she was good for 10 years, after which the battery would need to be replaced.
Heart valve disease
Your heart has four valves leading in or out of the heart chambers. If one or more doesn’t work well, you have Heart Valve Disease. You can be born with the defect (congenital) or it may develop over time as a result of aging or other damaging effects. Defective heart valves that develop later in life are usually associated with heart murmurs. It may cause a swooshing sound that is heard when listening with a stethoscope.
Heart valves can have three basic kinds of problems:
Regurgitation, or backflow, happens when the flaps of a valve don't close tightly. This allows the blood to leak backward. A common cause of regurgitation is prolapse, where the flaps of the valve flop or bulge back. Prolapse most often affects the mitral valve.
Stenosis happens when the flaps of a valve become thick, stiff, or stuck together. This prevents the heart valve from opening all the way. Not enough blood can pass through the valve. Aortic valve stenosis is a common type of stenosis. It affects the valve that controls blood flow into the large artery that carries blood out of the heart to the body.
Atresia happens when a heart valve did not form properly and does not have an opening for blood to pass through
Sometimes a valve can have both regurgitation and stenosis.
Heart valve disease can be treated by symptom reduction through lifestyle changes or medication. The valve can also be replaced or repaired through surgery.
Cardiomyopathy
Cardiomyopathy refers to a collection of disease conditions of the heart muscle tissue. It can alter the shape and reduce the function of the heart, especially the walls of the heart chambers. You may have heard stories about enlarged hearts, that is cardiomyopathy.
Watch this video for a quick overview.
Cardiomyopathy can either be inherited or caused by outside factors like alcohol abuse or infections. The condition tends to get worse over time, sometimes very quickly, and it can affect young children. It is a major contributing factor to other heart conditions like heart failure.
Heart Failure
Though the heart is robust and able to repair itself, permanent damage can and does happen. When damage occurs, the body will do things to compensate for the shortfall of function. If the unhealthy condition continues, even these measures will stop working. Eventually the heart starts to fail in its function to pump an adequate amount of blood around the body. This condition is simply called heart failure.
In heart failure the heart has not stopped, it is just not working well enough to meet the needs of the body. The overview is simple enough, but the details can be very complex. If you did an internet search on heart failure you would find it described as an ongoing problem (chronic) or it could happen suddenly (acute). It could be a right-sided failure (the heart is too weak to pump enough blood to your lungs to get oxygen). It could be the more common left-sided failure (the heart can't pump enough oxygen-rich blood out to your body). Or it could be both at the same time. It could be described as Diastolic (improper filling in the heart chambers- vs- Systolic (can’t pump hard enough). There are even math equations involved in describing heart failure (ejection fraction). We are going to let the doctors and nurses worry about all that and we’ll concentrate on what is important to In-home caregivers. How to recognize the symptoms and what to do about them.
When the heart can’t pump well, blood builds up in the blood vessels. Excessive fluids leaks into the surrounding tissues. The fluid starts to accumulate and how it shows as symptoms depend on which side of the heart is affected. Remember the anatomy lesson from earlier in the course. In right-sided heart failure, the blood can’t move from the body into the heart, so swelling of extremities and organs occurs. In left-sided heart failure, the fluid backs up into the lungs, and signs of drowning slowly start to show. It is easy to understand why heart failure is also called congestive heart failure (CHF). Though left-sided heart failure is more common, it often leads to right-sided heart failure as well.
The common signs and symptoms of CHF are:
Feeling short of breath, while doing normal activities or lying down. This may be one of the first symptoms caregivers will notice.
Fatigue or weakness even after rest.
Coughing or wheezing with white or pink blood-tinged mucus.
Crackling sound when breathing (Rales)
Swelling in the abdomen and rapid weight gain
Pitting edema from fluid in the ankles and lower legs.
Difficulty sleeping when lying flat.
Nausea and loss of appetite.
Swelling in the veins of the neck.
Needing to urinate often.
Angina
Difficulty in concentrating or decreased alertness
If you as a caregiver starts to see a collection of the above symptoms, it’s time to get your resident to the doctor. The doctor will probably ask you to modify the resident’s lifestyle and add heart medications, more about that later. If these measures seem to fail, then either a ventricular assist device (VAD) or a heart transplant may be needed.
Identifying the Problem
In-home caregivers are the first point of contact for the medical establishment at large. Often it is your observations that initially identify health problems that may have gone unnoticed, were misdiagnosed, or started to develop in the residents under your care. Knowing the risk factors and the common sign and symptoms of heart disease will help you focus your attention on where it needs to be.
Risk Factors
Not everyone develops heart disease. There are medical conditions, lifestyle choices, and family genetics that can increase the risk of having cardiac problems. Understanding why certain factors increase that risk will make it easier for caregiver to spot potential problems sooner.
High Blood Pressure- The long-term stress of high blood pressure in the cardiovascular system damages the arteries and organ tissues of the body. Arterial walls and the myocardium lose their elasticity and become stiff leading to loss of function. Damaged arterial walls create surfaces that make it easier for cholesterol or other fatty substances to attach, forming plaques and further reducing blood flow.
High Cholesterol Levels- Cholesterol is a lipoprotein. A waxy, fat-like molecule made by the liver. It can also be found in certain foods we eat. It is used by the body for many functions. There are different types of Cholesterol. LDL (low-density lipoprotein) is considered to be bad because it can cause plaque to form. Think of it as a fluffy cotton ball that sticks in the arteries and cuts off blood flow. HDL (high-density lipoprotein) is good cholesterol because it can scoop up LDL and therefore protects the heart.
Diabetes- Diabetics can have higher levels of glucose in the bloodstream. Glucose is a very reactive molecule. Glucose molecules can easily attach themselves to other molecules, disrupting their function and causing damage to structures in the cardiovascular system.
Obesity- Those who are extremely overweight are more likely to have multiple contributing heart disease risk factors. Including high LDL, low HDL, diabetes, high blood pressure, and lower activity levels.
Unhealthy Diets- Eating foods with high levels of saturated fats, trans fat, and cholesterol only increases their levels in the bloodstream. Foods high in salt increase the water level in the bloodstream (water follows salt). This leads to increased blood pressure. Refined carbohydrate food like bread and pasta leads to higher levels of glucose and increases the chance of diabetes.
Lack of physical activity- Inactivity leads to reduced muscle tone and less capable muscles in the heart and blood vessels. It also contributes to diabetes, obesity, and high blood pressure.
Alcohol- Too much alcohol can raise blood pressure, increase levels of triglycerides (a fatty molecule found in plaques) and damage the fine tissues of the cardiovascular system
Tobacco- Cigarette smoke contains harmful substances that damage the heart, lungs, and blood vessels. Nicotine increases blood pressure and hardens arteries. Carbon monoxide reduces the amount of oxygen in the blood.
Stress- Our body responds to stress by increasing blood pressure and heart rate. Too much stress can damage the heart.
Genetics- Defects in the cardiovascular system can be inherited. Heart disease in family members is important information to obtain.
Age and Gender- Tissue deterioration increases with age. The older you get the higher the risk of the structures of our bodies just wearing out. Starting at age 45, a man’s risk of heart disease begins to rise, while a woman’s risk begins to increase at age 55 (post-menopause).
Medical Conditions- Other pathologies can aggravate or weaken the cardiovascular system. A caregiver should increase their monitoring of cases of Chronic kidney disease, Autoimmune and inflammatory disease, Chronic pain conditions, or Infections like rheumatic fever and measles.
Medications- Harmful side effects are always a risk in medications. Watch for heart or blood pressure problems with the following drugs.
Nonsteroidal anti-inflammatory drugs
α1-blockers
Antimalarial agents
TNF-α inhibitors
Antineoplastic agents.
Oral Antifungal medications.
Minoxidil
Cocaine
Anabolic Steroids
Amphetamines (uppers)
Signs and Symptoms
Care home operators know their residents more intimately than any other medical professional. Who is better placed to notice abnormalities that may develop? In-home caregivers are not responsible for diagnosing heart diseases. You are responsible though in recognizing problems that need medical attention. That includes suspecting misdiagnoses when things just don’t add up right, (doctors are human too). Various pathological conditions have their own set of heart disease symptoms. You don’t have to worry about such fine details. You need to focus on what looks suspicious and report it to the doctor.
Keep a look out for:
Chest pain, chest tightness, chest pressure, chest discomfort, and sweating
Shortness of breath
Pain in the neck, jaw, throat, upper belly area, or back
Pain, numbness, weakness, or coldness in the legs or arms
Wheezing or crackly breaths
Difficulty sleeping while flat on their back or waking up early with feelings of breathlessness. Requests to be propped up with extra pillows
Pitting edema (when poked with a finger an indentation remains)
Complaints of weakness or difficulty completing normal activities
Fainting or dizzy spells
Complaints of palpitations (pounding, racing, or fluttering heartbeats)
(Jugular Vein Distention)
Unexplained quick weight gain and or increases in girth around the stomach
Large neck veins (Jugular Vein Distention)
Increase in nighttime urination
Pale grey skin or blue-tinged lips or fingertips
Unexplained wet-sounding cough
Frequent nausea
General complaints of feeling unwell or ill at ease
Pains felt deep in the legs (deep vein thrombosis)
Feeling for irregular heart rate.
Place two fingers on either side of the windpipe or in the groove neck to the bone just below the wrist. Check your own pulse to get a feeling of what is normal then check the resident.
If you are unsure if you could feel an irregular heart rate check this video out.
High Blood Pressure
Taking blood pressures at home has become easier with advancements in automatic blood pressure machines. Due to natural variations in conditions, you never get excited about single readings. In-home caregivers need to concern themselves with changes in patterns over time.
Systolic
Diastolic
Normal
Less than 120
Less than 80
Prehypertension
120-139
89-89
Hypertension
140 or higher
90 or higher
High Cholesterol
You can buy over-the-counter cholesterol tests, but I think it’s a waste of your time and money. The county regulators would probably frown on the idea and the doctor would take his or her own tests anyway. Caregivers can ask for copies of the doctor’s test or even see them online now.
Cholesterol levels indicating high risk
Good
Bad
HDL
More than 60mg/dL
Less than 40mg/dL
LDL
Less than 100mg/dL
More than 160mg/dL
Total Cholesterol
Less than 200mg/dL
More than 240mg/dL
Working with the doctor
So you have seen enough bad signs to start having suspicions. Now what do you do? Just calling the primary care physician is ok but you are a professional. You need to take it up a notch. Trust me on this. Care provider efforts put in here will give you great benefits down the road. Your reputation will grow. Working with the doctor will get easier. You will get faster results. Your resident and their family will trust you more and you will experience fewer problems in caregiving. To achieve these benefits, I recommend the following.
Make a record of your observations. Things in writing are unusual and are paid attention to.
If you know what you are doing, use medical terminology. Buy yourself a medical dictionary if you have to.
Include measurements. Doctors are scientists by training and they like lots of data. Measurements can be a little as the frequency of occurrence of symptoms. For example, had dizziness for about a minute upon standing three times this week and had fainting spells twice this month. Increase in weight of 10lbs in one week. Had to use 2 extra pillows at night to help in sleeping comfortably. B/P while sitting was 140/90, 148/92, 150/90 taken just after breakfast.
Ask lots of questions. If you have suspicions phrase them in the form of a question. Do you think the wheezing I hear is from congestive heart failure? Can this fainting be caused by arrhythmia? Can these complaints about chest heaviness be angina? (see what I did there with the medical terminology?)
Develop a partnership with the doctor. Ask him what he needs to help him do his job. If you need things yourself do not hesitate to ask.
Let the patient answer the questions. The doctor is used to working one on one directly with the patient. Do not be overbearing or condescending toward the patient, it makes you look bad. You may have to supply clarifications or missing info though. Come on too strong and the doctor will get annoyed with you.
Make friendly comments to the doctor’s staff. Joking with the staff creates a cooperative environment while keeping things respectful with the doctor.
Strive for understanding. Keep communicating until everyone is comfortable with what is going on. Translate medical jargon into everyday language for the patient. Parrot back to the doctor what you think he or she means about key points and instructions. This will help to ensure you are understanding things correctly and show that you are taking the matter seriously.
When calling the doctor's office, it is easier to talk directly with the nurse than it is with the doctor. Working just with medical assistants is questionable at best. If it is important, ask for a call back from the doctor or at the least insist on talking with a nurse.
Pushing for a specialist
Becoming a partner with the primary care physician (PCP) is all well and good, but sometimes you got to go beyond them and get a specialist. Cardiologists are the experts when it comes to all things heart-related. They know all the subtleties of symptoms and the tricks of treatments. They will work with you and help your resident have as normal a life as possible despite their heart problems. As the advocate for your resident that is what you are supposed to do.
Real-world example. Do you remember the story about my Mother in law’s heart problem from earlier in the course? I knew that something was amiss medically, but I lived an entire state away and couldn’t do much. I finally got fed up and took the time to go where she lived. I thought I could work with the doctor and fix things. Frustratingly, the doctor was entrenched in thinking the problem was caused by a drug side effect. I gave up. When I moved her here, I got her a new PCP and told him everything. The first thing he did was to get her to a Cardiologist. I was skeptical at first, thinking “great a totally new guy I have to work with”. I was a tad bit tired of doctors by this point. Well, you know the rest of the story. After doing the research for this CE course, I now know that the cardiologist knew all the right tests to use to make the correct diagnosis. I could have saved so much effort and worry if I’d known that while working with the first doctor. Sometimes hindsight can slap you right in the face and wake you up.
Testing for Heart Disease
I hope that you can see that even an old dog like me can learn new tricks. Rarely does the outward signs point to an obvious conclusion. Usually, more tests are required to locate the hidden signs that can change the diagnosis. But nobody likes going to the doctor and taking more tests. If you have a fearful or uncooperative resident, reassure them that most screening tests for heart disease are done outside of the body and are painless. Tell them that the more information a doctor has the better decisions they can make.
The doctor may choose to give one or more of the following tests:
Electrocardiogram (ECG or EKG) makes a graph of the heart’s electrical activity as it beats. This test can show abnormal heartbeats, heart muscle damage, blood flow problems in the coronary arteries, and heart enlargement.
Stress test (or treadmill test or exercise ECG) records the heart’s electrical activity during exercise, usually on a treadmill or exercise bike. If you are unable to exercise due to arthritis or another health condition, a stress test can be done without exercise. Instead, you can take a medicine that increases blood flow to the heart muscle and shows whether there are any problems in that flow.
Nuclear scan (or thallium stress test) shows the working of the heart muscle as blood flows through the heart. A small amount of radioactive material is injected into a vein, usually in the arm, and a camera records how much is taken up by the heart muscle.
Echocardiography changes sound waves into pictures that show the heart’s size, shape, and movement. The sound waves also can be used to see how much blood is pumped out by the heart when it contracts.
Coronary angiography (or angiogram or arteriography) shows an x-ray of blood flow problems and blockages in the coronary arteries. A thin, flexible tube called a catheter is threaded through an artery of an arm or leg up into the heart. A dye is then injected into the tube, allowing the heart and blood vessels to be filmed as the heart pumps. The picture is called an angiogram or arteriogram.
Ventriculogram is frequently a part of the x-ray dye test described before. It is used to get a picture of the heart’s main pumping chamber, typically the left ventricle.
Intracoronary ultrasound uses a catheter that measures blood flow. It creates a picture of the coronary arteries that shows the thickness and other features of the artery wall. This lets the doctor see blood flow and any blockages.
Carotid doppler ultrasound uses sound waves to detect blockages and narrowing of the carotid artery in the neck, both of which can signal an increased risk for heart attack or stroke.
Electron-beam computed tomography is a superfast scan that provides a snapshot of the calcium buildup in your coronary arteries.
Magnetic resonance imaging (MRI) is a scan using magnets and computers to create high-quality images of the heart’s structure and functioning. It is often used to evaluate congenital heart disease. The test can also detect severe blockages in coronary arteries in people who are having unstable angina or a heart attack, thereby allowing immediate treatment to restore blood flow to the heart.
Holter monitoring. A Holter monitor is a portable ECG device that's worn for a day or more to record the heart's activity during daily activities. This test can detect irregular heartbeats that aren't found during a regular ECG exam.
When someone experiences bad news, it is only human to complain “Why Me!” Barring bad luck events like the defective genes you were born with; the usual answer is, “because you made too many risky choices and now it’s catching up to you”. If you want to avoid bad consequences make good choices. If the damage has already happened, then stop doing the things that will make a bad situation worse. In-home caregivers are in the perfect position to turn things around for the resident with heart disease.
Modifying risk factors
Smoking- As we have already covered, smoking puts stress on the heart in many ways. Care homes need to have clearly written anti-smoking policies. If you have to allow smoking, (mental health patients often use nicotine as self-medication therapy so it’s really hard to stop) then you have to control the secondhand smoke. If the caregivers themselves smoke, then you are opening yourself up to “caused harm to heart disease patient” lawsuits.
If you or a resident are trying to quit, the number one recommendation I can make is to make the environment extremely uncomfortable to smoke in. No comfy chairs to sit in, no ashtrays (make them dig for an old can in the garbage) no after-dinner smoking sessions. The good news is that quitting smoking will immediately and significantly reduce the risk of further heart disease complications.
High Blood Pressure (HBP)- You can’t feel HBP until after it’s too late. You have to rely on BP monitoring and take HBP readings seriously. Taking your resident's BP regularly might not be a bad idea. If you do, keep a record of the readings and let the doctor see it periodically.
You can reduce HPB by:
Losing weight, Just 5-10% weight loss starts to protect the heart.
Exercising, In a care home, start by taking scheduled walks. Work up to 30 minutes on most days.
Stop drinking alcohol
Reduce salt intake- The Dash diet might be worth looking into.
Here is a good intro to the Dash Diet
High Cholesterol
You lower cholesterol blood levels by eating healthier, period ‘nuff said.
Cook from scratch. It’s cheaper (more profitable), looks good to potential new clientele, and makes the current residents more satisfied with staying in your home. It doesn’t take any talent. It just takes practice, planning, and shopping for the right foodstuffs. Include foods high in fiber, but low in saturated fat, trans fat, total fat, and cholesterol. The days of deep-fried pig fat on a stick are gone. Fat may be flavor, but it’s also pain and misery to heart disease sufferers.
If you want to take a short cut, look into the DASH diet. It will cover reduced salt and fats. Here again, the key to easy implementation starts with buying the right foodstuffs. Make a menu then use what is on it to make a shopping list.
Stress
Moving into your home and dealing with change can be stressful for the resident. But after that, a reduced stress environment is totally doable. I recommend concentrating on creating clean, tidy and quiet surroundings, and a stable predictable schedule. Predict stressful situations and take steps to prepare for them. And for heaven’s sake, reduce the number of choices that a resident has to make.
Fluids
Proper hydration is important, but you don’t want to aggravate the pathophysiology of congestive heart failure, high blood pressure, or any severe heart disease condition. If you have residents with any of these disorders consult with the doctor about how much fluids to give. Don’t forget what’s on the menu when totaling fluid intakes.
It probably wouldn’t be a bad idea to weigh the patient regularly and put a cloth tape measurer around the waist every so often. An increase of 2-3 lbs a day or 5 lbs a week are red flags and the doctor needs to be notified. Record the info and give it to the doctor when needed.
Sleep
Sleep disturbances are a red flag in heart disease patients, especially congestive heart failure. The extra fluids easily flow into the lungs when lying flat. The extra fluid can also pool in the kidneys, increasing the need for nighttime urination. Extra pillows can help but foam wedges are better. I have even heard of caregivers putting the head of the bed on bricks to angle up the entire bed.
Complaints
Pay attention to complaints and don’t dismiss them out of hand. Complaints may be caused by new symptoms or worsening conditions that are starting to manifest themselves.
Misc.
The more ill a patient is, the greater the need to get all their shots.
Control diabetes and you control heart disease and vice versa. The therapies overlap each other considerably
Mini Pedalers and hand weights are an easier-to-use exercise option in care homes. Consult with the doctor before anything strenuous.
All of the above measures could be utilized for the entire household as part of a heart disease prevention strategy.
Heart Disease Therapy
Medications
There are a wide variety of medications that a prescriber can utilize in heart disease therapy to control risk factors or reduce symptoms. To make it easier for you we will list them by drug class. But first, you need to know some pharmacology terms and you also need to remember some of the stuff we covered in the anatomy and physiology sections.
Vasodilators- drugs that reduce blood pressure by opening up the blood vessels. They usually do this by relaxing the smooth muscle that constricts around the vessel. A common side effect is orthostatic hypotension (the dizziness and falling side effect)
Orthostatic hypotension (OH) or postural hypotension- Blood rushing away from the brain when you stand or sit up. The remedy is getting up slowly or in stages, pausing in between actions.
Vasoconstriction- Tightening of the smooth muscle around blood vessels. Naturally the result of a nerve impulse.
ACE inhibitors
Vasodilator with names often ending in -pril (lisinopril). They work by stopping the body from producing a chemical that narrows blood vessels. It lowers HBP, reduces heart attacks, heart failures, and protects the kidneys in diabetes. Helps excrete some sodium. Watch for OH. May cause a constant dry cough.
ARBs Angiotensin II Receptor Blocker
Works similar to an ACE but with no cough.
Beta Blockers
Blocks the effect of epinephrine and norepinephrine causing the heart to beat more slowly and with less force, which lowers blood pressure. Also is a Vasodilator. Used to treat HBP, arrhythmias, and anginas and reduces the chance of a heart attack. Watch for OH. Their names can end in -olol (metoprolol)
Calcium Channel Blockers
Helps block the signal that causes certain nerves to fire. Reduces vasoconstriction and slows the heart. Used to treat HBP, arrhythmias, and anginas and reduces the chance of a heart attack. They are vasodilators so watch for OH.
Diuretics (water pills)
Drugs used to fight fluid buildup. Lowers HBP and reduces pitting edema. Loop directs like Lasix may cause low potassium problems like confusion or leg cramps. Diuretics may work too well so watch for dehydration signs. Giving them later in the day will cause extra urination at night so dispense them in the AM. Watch for OH
Digitalis
Helps the heart beat stronger and slower. Lots of side effects and interactions with other drugs. Watch for Nausea and Vomiting. If the resident starts to have vision changes like yellow or greenish halos, stop the digitalis and call the doctor right away.
Anticoagulants and antiplatelets (blood thinners)
Prevents harmful blood clots. Used to reduce heart attacks and angina. Includes low-dose aspirin and warfarin also called the bruiser med. Be prepared to deal with ugly bruises at the mere grip of the wrist or brush of the skin. If there is too much bruising call the pharmacy or doctor. The dose might be too high. Might have to watch the consumption of certain foods like grapefruit.
Nitrates and Nitroglycerin
Drugs that relax blood vessels and promote blood flow by breaking down into Nitric Oxide. Used to prevent heart attacks and relieve angina. Nitroglycerin can evaporate from pills if left out or place under heat. If the pills don’t tingle when used, they have lost their potency. Can cause major headaches. Used as a rescue med, the dosage is prn pain, up to 3 times- 5 minutes apart before calling 911. There may be new guidelines coming out so talk to the doctor.
Cholesterol-lowering drugs
Drugs that lower LDL but sometimes may increase HDL. A popular family of these meds are the satins like atorvastatin (Lipitor). They may cause muscle pain or weakness. Call the doctor if it happens. May also cause memory loss in certain patients. Grapefruit will interfere with statins.
Managing Angina
Managing angina can be summed up in a single sentence, “avoid the triggers”. Triggers are anything that makes the heart work harder. Common activities notorious for causing angina pain are a sudden increase in physical activity, emotional stress, cold weather, eating a big meal, high blood pressure, being overweight, cigarette smoking, and long bouts of constipation strain. Combining harmful activities like going out in cold weather after the thanksgiving feast or holding your breath while lifting is a no-no. Caregivers should start exercise programs gradually. If angina is occurring frequently, keeping an angina diary will help identify potential triggers to avoid in the future.
Heart attack Management
I know that most of you have had CPR training, so I’ll just put up a reminder list of heart attack warning signs.
Chest discomfort or angina
Discomfort in the arms, back, neck, jaw, or stomach
Shortness of breath
Lightheadedness
Breaking out in a cold sweat
Surgery
Surgery as therapy is essentially modifying the problem areas of the cardiovascular system. They may include:
Coronary Angioplasty (“Balloon” Angioplasty)- inflating a tiny balloon in an artery to increase blood flow.
Plaque Removal- atherectomy (shaving off the plaque) or laser angioplasty (burning off the plaque)
Stent Placement- inserting a tiny wire mesh to keep the artery open.
Coronary Bypass Surgery- basically replumbing around the problem area.
Cardiac Rehabilitation
Cardiac Rehabilitation is a supervised program that includes a team of specialists working on all aspects of heart disease recovery. The team includes the doctor's office, exercise and nutrition specialists, physical therapists, and counselors. In-home caregivers should find out who’s in charge and fight to be included in the program. You might have to do some educating to let them know who you are and what you can do. I recommend that you tell them that you are the superman of facilitation and the captain of get ‘er done.
Conclusion
Heart disease can drastically alter the life of your residents. Your goal as the In-Home caregiver and patient advocate is to do what is necessary to help the resident return to as normal life as possible. You can help them understand what is going on and what things they need to do. You can help them manage their therapy, medication, and lifestyle choices. You can also provide a supportive stress-free environment to live in, which might be the most important thing that you can do.
Vishal Punwani. What is coronary artery disease? | Circulatory System and Disease | NCLEX-RN | Khan Academy. Khanacademymedicine, Oct 22, 2014 https://www.youtube.com/watch?v=EATkbpqlxvc
Credit Hours 1 - Approximate time required: 60 min.
Educational Goal
Discuss aspects of emergency plan implementation.
Educational Objectives
Review the difficulties when faced with an emergency
Tell what is to be done in the first 3 minutes of a disaster
Tell what is to be done in the first 3 days of a disaster
Tell what is to be done in the first 3 weeks of a disaster
Suggest 12 ideas that will assist in handling emergencies in care homes.
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.
The 1st-3s in Emergency Preparation
I assume you have had enough courses and lessons on how to make an emergency plan. Let’s also assume you are bored to death at the thought of having to do another Emergency Prep course. So, let’s take a different approach. Let’s go over some ideas on how to implement your plan because doing a plan is always different from making a plan. Let’s set the stage for our discussion.
The first three difficulties of Emergency Preparedness implementation
The first three difficulties of implementing an Emergency Preparedness plan are:
Disasters by their very nature are unpredictable. It is impossible to predict every possible emergency that may occur in your home. The best-laid plan will never be able to account for every variable. You can be prepared though with a flexible plan that will allow you to react appropriately to any situation that may arise.
Resources are finite in your home. You will not be able to resolve every situation that may arise by yourself. Often the disaster itself will restrict resources that you counted on. For example, a flood can limit outside employees and families from coming to your aid. But you can tie it into other resources the community has to offer, but only if you know about them.
Time is also limited during emergencies. There will not be enough time to think through the situation and decide on an appropriate course of action. Also, let’s face the facts- brains have a tendency to turn off during disasters, just when you need them the most. Having a well-practiced plan of action that you can fall back on reduces the stress caused by limited time restraints.
With these difficulties in mind just how solid is your emergency plan? If you’re planning on everything going to plan then you are planning to fail. It’s time to pull out that plan and take a critical look at it.
If you are thinking I am going to tell you something magical that will make you prepared for any emergency, sorry it ain’t gunna happ’m capt’m. That’s your and the rest of the staff’s job. My job is to get you to look critically at your plan and beef it up with a few good ideas.
Suggested idea #1 Always be willing to rewrite your plan
Convert your typed-out plan into an outline. Add lots of space between each point. Then be willing to add notes in the space.
Go through the plan and ask what if things don’t go as anticipated. Then either write a plan B on each point or add enough flexibility to handle unforeseen circumstances.
When you have emergency disaster drills or an actual emergency take note of what goes wrong. If researched properly, problems are where being prepared for the unexpected “gold nuggets of wisdom” are hidden. Messed-up plans are excellent teachers if you pay attention to what they are saying.
Make your plan a living document. Always have space in your outline and a willingness to add to it as good ideas occur, or when bad outcomes force you to rethink your plan.
The 1st three minutes of a Disaster
Have you got your plan out yet? Good, let us do a linear time analysis of the details as you implement your plan in your head. Think about what will happen as time progresses compared to what should happen. Let’s start with the first three minutes of a disaster.
Determine who is in charge
Gather information
Decide what action path to take
Start acting out the plan
From what I have seen of the emergency action plans out there in regard to these four items, most of you will be thinking, “Huh! What the freak is he talking about?” This is when things start falling apart, right at the beginning. You didn’t think through how your wonderful plan will actually be used. Without thinking through how you implement the plan you will be running around in circles trying to decide on what to do on too many things.
Suggested idea #2 Who’s in charge
Write into the plan a way to determine who is in charge. Base it on experience, ability, availability, or whatever you want. Then designate who’s second in command if the first guy is taken out of the picture. Create a Leader’s folder that has the written disaster plan and the location of the needed supplies for various parts of the plans. Make it easy to find and complete so you can grab it and go in a few seconds.
Suggestion idea#3 Where do you go for information
Include in your Leader’s folder where to look for Good information. Weather Channel, Police, Fire Department, American Red Cross, County Government Homepage under emergency management, etc…
Download the FEMA app here. https://www.fema.gov/about/news-multimedia/mobile-products
Suggested idea #4 A Decision Tree
A decision tree is a specific type of flow chart used to visualize the decision-making process by mapping out different courses of action, as well as their potential outcomes. You can draw one by hand or look up a free template on the computer.
You can really drive yourself crazy by filling one of these things out. I recommend keeping it simple. Stick to the big questions. Add just enough details to make the tool useful but easy to use.
Final thoughts on the 1st three minutes. The principle I’m going for here is time management. In an emergency, minutes count. Think about what will be needed and streamline the actions. Have as much ready beforehand so you can concentrate on the critical stuff. Take a minute to write down notes on your disaster plan while the thoughts are fresh.
The First Three Days
It has been said that you have the freedom to choose actions, but you don’t have the freedom to choose the consequences of those actions. I would like for you to now ask the following questions:
What detail did I miss in my original plan that needs to be taken care of in advance?
What are the most likely consequences of the action steps in my plan?
What do I do if things don’t go as expected? How can I plan around things going wrong?
I admit this is a hard thing to do. You’re not a fortune teller. You can’t see into the future. But you can visualize what things might be like once you have made your choices in a disaster.
For example.
If you have chosen to evacuate,
Where will you end up?
How will you get the things you need once the supplies you brought with you are used up?
What special items will you need that will not be at the shelter where you end up at?
If you have chosen to shelter in place,
How will you get fresh supplies?
What adjustments will be needed to make supplies stretch out?
What will not be available that I need? (electricity, meds, water, etc..)
What will happen if I am still forced to evacuate?
How will I get extra help if needed?
Suggested idea#4 Bug Out Bags
If you are sheltering in place and there is still the possibility that you will have to leave, prepare bug-out bags for each person in the home. Hang them on the end of each bed. The idea is you can grab them and go at any given moment of the emergency. They would include clothes, shoes, specialty equipment supplies, a whistle, a space blanket, a patient info folder that lists meds, allergies, medical conditions, insurance, family contact, care plan, etc… And if you do have to “Bug Out” don’t forget their pillows.
Suggested idea#5 Wrist Id bands
There is a reason why hospitals put wrist id bands on their patients. If you are evacuating to who knows where, wouldn’t it be a good idea to do the same? Keep a supply of them in the disaster plan folder.
Suggested idea#6 Check expiration dates regularly
The bug-out bag is in addition to you 72-hour kit that you have prepared. You do have a 72-hour kit already made up…. Right! You have gone thru them and replaced outdated items on a regular basis….Right! Of course, you have because you are taking this very seriously…..Right? Have you ever tasted outdated emergency food or water? You will not die but they’re very nasty. Let’s not even talk about flashlight batteries and trying to see in the dark. See what I mean about consequences and things not going as expected?
Suggested idea#7 Car Kits
72-hour kits can be augmented by emergency kits in the expected transportation vehicles that will be used. Stuff that is needed but is too bulky or dangerous for the 72-hour kit. Things like extra water, flares, blankets, fuel for cooking, duct tape, rope, cooking equipment, lantern, bucket, etc. Think like you are going camping and bring what you need.
You can store them in the car or in an easy-to-grab plastic tote. Old Boy Scouters call these totes, “Action Packers”
Suggested idea#8 Shutting things off
If you are evacuating have a designated shut-off person in your plan. Train them in advance on how to turn off the gas, water, and electronic devices Also show them where special shut‐off tools are stored. If you need special tools get them. If you don’t know how to shut stuff off, you can get training from the utility company or tradesmen in the field.
Suggested idea#9 Entertainment
Plan on how to entertain the residents. Keeping their attention focused away from the chaos around them will help keep things calm and easier to manage
The First 3 Weeks
Heaven forbids that an emergency will last more than a few days. If they do, you will have to switch your mindset from mere survival to maintenance issues. Resupply will be a major concern whether you are at home or not. Water filters with enough capacity will be very important at this time. You will also have to decide when you pass the torch of responsibility for those you care for to someone else. Who will that be for each person and how will it happen? Most often that will be family members but what will you do if the family member is caught up in the disaster too? For the tough cases contact the county licensor. They will be a great help with these topics. Of course, you can coordinate with the disaster relief personnel during the disaster. Put these contacts into your emergency plan as well as in your Leader’s file. Don’t forget to tell the appropriate county officials where everyone went to. If you are prepared enough, these issues will not happen. But we are talking about what to do when things don’t go as expected, aren’t we?
Suggested idea#10 Disaster relief personnel
Add into your emergency plan the step of finding out who the top disaster relief personnel are for this specific disaster, and how to contact them.
Suggested idea#11 Facility agreements
Contact larger care institutions like hospitals and nursing homes in your area and enter into emergency care relief agreements. Get them in writing so you can show them to the person in charge if needed. To grease the wheels of the deal, offer to volunteer your services where needed.
Suggested idea#12 Generators
Generators are great at helping you be prepared for the unexpected. With a generator, sheltering in place becomes the easy solution for a lot of unexpected problems that might occur. In my opinion, it is well worth the extra cost. It also is a good selling point for potential new residents. If you go with the generator option, be forewarned that you will have to get an electrician to install special connections to your home's electrical supply. You will also have to store extra fuel, and of course, it will take practice using it. I would include instructions for its use in the emergency plan folder.
Conclusion
I hope you enjoyed this different take on emergency preparedness. How did your plan fair? Poked a few holes in it didn’t yah? That’s okay because you are now going to make your plan a living document that will only get better as you change it over time. The small efforts you take now will save you tons of grief and effort when things go to heck during a disaster.
Credit Hours 2 - Approximate time required: 120 min.
Educational Goal
Discuss aspects of clinical depression and its management.
Educational Objectives
Define what clinical depression is
List the signs and symptoms of depression
Discuss the risk factor for developing depression
Explain therapeutic options
Cover the drugs used in thyroid therapy
Tell how In-home caregivers can manage affected residents
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.
Well That’s Certainly Depressing
Residents in care homes are always at greater risk for depression. The stress of changing living environments, health issues, and reductions in personal freedoms can make anyone depressed. Good caregiving techniques can reduce or eliminate such factors. But when depression remains or returns, what does an In-home caregiver do? When does regular unhappiness turn into clinical depression? Can clinical depression be “cured”? We will explore these and other questions in this course on depression.
Depression, what is it?
“Sometimes we eat the bear and sometimes the bear eats us”.
Our lives are full of stresses. When those stressors become overwhelming it is natural to get feelings of depression. I believe that these “down” feelings are a defense mechanism that slows us down and protects us from even greater harm. Depressive feelings slow us down to protect us from overextending ourselves, both physically and mentally. It helps us reflect onwhat is transpiring in our lives. In those times of reflection, we can find the solutions that enables us to cope with what is going on around us. After a “good cry” often we feel rested and cleansed. We start to feel better about our circumstances and can jump back into the fight.
Our body's depression processes are multifactorial and are not fully understood. Studies show that brain structure, genetics, biological, environmental, and psychological factors can play a role in depression. We do know that there are a number of hormonal responses and neurochemical chemical changes involved. In layman's terms, there are chemical start and stop buttons that our bodies use to regulate the depression reaction process. As we move through life, these buttons can be pushed or triggered by the circumstances that we experience. Depressive symptoms can be triggered as a side effect of medication. The pathophysiology of diseases can trigger the depression response and is seen as a symptom in many diseases. There are also those whose depression-causing mechanisms get stuck or are broken and they experience what we call “clinical” depression.
What are the Types of Depression?
With so many causative factors involved, it is only natural that there are different types of depression. Common forms of depression are:
Major Depression, which includes symptoms of depression most of the time for at least 2 weeks. Episodes typically interfere with one’s ability to work, sleep, study, and eat.
Persistent Depressive Disorder (dysthymia), which often includes less severe symptoms of depression that last much longer, typically for at least 2 years.
Perinatal Depression, which occurs when a woman experiences major depression during pregnancy or after delivery (postpartum depression).
Seasonal Affective Disorder, which comes and goes with the seasons, typically starting in late fall and early winter and going away during spring and summer.
Depression with Symptoms of Psychosis, which is a severe form of depression where a person experiences psychosis symptoms, such as delusions (disturbing, false fixed beliefs) or hallucinations (hearing or seeing things that others do not see or hear).
Depression is a disorder that is more than just feeling blue. It is a medical condition that has observable signs and symptoms which range from mild, to moderate to severe. Common symptoms of depression include:
Persistent sad, anxious, or “empty” mood
Feelings of hopelessness or pessimism
Feelings of irritability, frustration‚ or restlessness
Feelings of guilt, worthlessness, or helplessness
Loss of interest or pleasure in hobbies or activities
Decreased energy, fatigue, or being “slowed down”
Difficulty concentrating, remembering, or making decisions
Difficulty sleeping, early morning awakening, or oversleeping
Changes in appetite or unplanned weight changes
Aches or pains, headaches, cramps, or digestive problems without a clear physical cause that do not ease even with treatment
Suicide attempts or thoughts of death or suicide
Increase in purposeless physical activity (e.g., inability to sit still, pacing, handwringing) or slowed movements or speech
Unexplained physical problems, such as back pain or headaches
It may make it easier for a caregiver to have a list of recognizable symptoms but in depression, it is not so cut and dry. Though the same chemical buttons are being pushed, how we respond to those chemical processes can be different in each patient. Outward signs can even change as the patient ages and develop different coping strategies.
Children with depression may be anxious, and cranky, pretend to be sick, refuse to go to school, cling to a parent, or worry that a parent may die.
Older children and teens with depression may get into trouble at school, sulk, be easily frustrated‚ feel restless, or have low self-esteem. They also may have other disorders, such as anxiety and eating disorders, attention-deficit hyperactivity disorder, or substance use disorder. Older children and teens are more likely to experience excessive sleepiness (called hypersomnia) and increased appetite (called hyperphagia). In adolescence, females begin to experience depression more often than males, likely due to the biological, life cycle, and hormonal factors unique to women.
Younger adults with depression are more likely to be irritable, complain of weight gain and hypersomnia, and have a negative view of life and the future. They often have other disorders, such as generalized anxiety disorder, social phobia, panic disorder, and substance use disorders.
Middle-aged adults with depression may have more depressive episodes, decreased libido, middle-of-the-night insomnia, or early morning awakening. They also may more frequently report having gastrointestinal symptoms such as diarrhea or constipation.
Older adults with depression commonly experience sadness or grief or may have other less obvious symptoms. They may report a lack of emotions rather than a depressed mood. Older adults also are more likely to have other medical conditions or pain that may cause or contribute to depression. In severe cases, memory and thinking problems (called pseudodementia) may be prominent.
It has been shown that men and women tend to show depression symptoms differently. Depression in women may occur earlier, last longer, and be more likely to recur than depression in men.
Men are likely to have:
changes in appetite
fatigue
low self-esteem
sleep disturbances
misusing alcohol or other substances
irritability, frequent outbursts, or “explosive” anger
risk-taking (such as reckless driving or substance-impaired driving)
escapism (e.g., working late, spending more time at the gym, playing video games for hours)
Women have tendencies to:
Ruminate over their circumstances
Have depressive episodes associated with stressful life events and be more sensitive to seasonal changes.
Experience guilty feelings and attempt suicide, although they actually kill themselves less often than men.
Be more likely to be associated with anxiety disorders (especially panic and phobic symptoms) and eating disorders.
Though we can all recognize the symptoms of depression it takes a skilled doctor to make a depression diagnosis. For a doctor to make a diagnosis of depression, a patient must have at least five depression symptoms every day, nearly all day, for at least 2 weeks. These symptoms must be a change in previous levels of functioning and one of the symptoms must be a depressed mood or a loss of interest or pleasure in almost all activities.
Are Their Risk Factors for Developing Depression?
Depression can affect anyone, even a person who seems to live in the best of surroundings.
According to the Anxiety and Depression Association of America “At any point in time, 3 to 5 percent of people suffer from major depression; the lifetime risk is about 17 percent.”
The National Institute of Mental Health estimates that figure to be even higher “In 2017, around 17.3 million adults age 18 or older in the U.S. had experienced at least one major depressive episode in the last year (6.7% of adults in the U.S)”
Some factors that appear to play a role in developing a depressive episode include:
Biochemistry: Differences in certain chemicals in the brain may contribute to symptoms of depression.
Genetics: Depression can be inherited and run in families. It has been shown that if one identical twin has depression, the other has a 70 percent chance of having the illness sometime in life.
Personality: People with low self-esteem, who are easily overwhelmed by stress, or who are generally pessimistic appear to be more likely to experience depression.
Environmental factors: Continuous exposure to violence, neglect, abuse or poverty may make some people more vulnerable to depression
Physical: Patients experiencing long-term physical ailments can have their coping mechanisms overwhelmed or depleted and develop depression symptoms.
Disclaimer: I’m a pharmacist, and I tend to see everything as chemical reactions. I wrote this course with that in mind because I think it makes it easier to understand. But I admit I am a chemical geek. I acknowledge that there are other ways of looking at the data that may be used in understanding depression cases. So don’t get too caught up in seeing all things mental health as mixed-up brain chemicals. That can be as harmful as thinking that all mental health cases are a result of a weak character.
How Is Depression Treated?
Even though depression is a very common occurrence fortunately it is among the most treatable of mental disorders. Between 80 and 90 percent of people with depression eventually respond well to treatment. Almost all patients gain some relief from their symptoms and develop some coping skills. Broadly categorized, treatments involve creating a supportive environment, psychotherapy, medication, and brain stimulation therapy. Providing support can be applied to all cases while psychotherapy and medication can be applied alone or in combination. Brain stimulation is usually reserved for treatment-resistant cases.
Creating a supportive environment
Creating a supportive environment as therapy for depression is trying to reduce stressors that may trigger or aggravate depression symptoms. It is also taking care of the activities of daily living so patients can concentrate on coping with their illness. This is what care homes do best. There are ways to fine-tune what you do to be more effective in managing depressive patients…. more about this later.
Psychotherapy
I have had no training or experience in psychotherapy, so as not to lead you astray I will just quote from the National Institute of Mental Health website.
“Psychotherapy (also called “talk therapy” or “counseling”) teaches individuals with depression new ways of thinking and behaving and helps with changing habits that contribute to depression. Most psychotherapy occurs with a licensed, trained mental health professional in one-on-one sessions or with other individuals in a group setting. Two effective psychotherapies to treat depression include Psychotherapy (CBT) and interpersonal therapy (IPT). The use of older forms of psychotherapy, such as dynamic therapy, for a limited time also may help some people with depression.
With CBT, people learn to challenge and change unhelpful thinking patterns and behavior to improve their depressive and anxious feelings. Recent advances in CBT include introducing mindfulness principles and the development of specialized forms of therapy targeting particular symptoms, such as insomnia.
IPT focuses on interpersonal and life events that impact mood and vice versa. The goal of IPT is to help people improve their communication skills within relationships, establish social support networks, and develop realistic expectations to help them deal with crises or other issues that may be contributing to or worsening their depression.”
Let me augment this explanation with a quote from the American Psychiatric Association website.
“Psychotherapy, or “talk therapy,” is sometimes used alone for the treatment of mild depression; for moderate to severe depression, psychotherapy is often used along with antidepressant medications. Cognitive behavioral therapy (CBT) has been found to be effective in treating depression. CBT is a form of therapy focused on problem-solving in the present. CBT helps a person recognize distorted/negative thinking with the goal of changing thoughts and behaviors to respond to challenges in a more positive manner.
Psychotherapy may involve only the individual, but it can include others. For example, family or couples therapy can help address issues within these close relationships. Group therapy brings people with similar illnesses together in a supportive environment and can assist the participant to learn how others cope in similar situations.
Depending on the severity of the depression, treatment can take a few weeks or much longer. In many cases, significant improvement can be made in 10 to 15 sessions.”
Medications
Our brains run on neurotransmitters. They are chemicals that trigger the electrical signals in our nervous systems. These signals tell our body what to do, including what to think. As stated earlier, the cause(s) of depression is not fully understood. One theory states that its cause is an imbalance of neurotransmitters in the central nervous system. Medications used to treat depression target these imbalances and are called antidepressants.
Antidepressants
Fair warning- I’m going to go a little deeper into the chemistry than normal. Hanging in there will help you get to a higher level of understanding. It will help you function a little closer to other healthcare providers that have college degrees.
There are three chemicals called monoamines that have been shown to be involved in mood regulation.
They are:
Dopamine- It is involved in decision-making, motivation, arousal, and the signaling of pleasure and reward
Norepinephrine- It is involved in alertness, motor function, and regulation of blood pressure and heart rate in response to stress
Serotonin- It is involved in regulating mood, appetite, sleep, memory, social behavior, and sexual desire
It has been shown that many patients who suffer from bouts of depression have low levels of these neurotransmitters. One would think that giving patients more of these as medication would solve the problem. Unfortunately, that messes up a lot of other functions that use these same chemicals. Too many side effects are the result. So the medication strategy has switched to helping the body utilize what neurotransmitters that are already there. Let me explain.
Nerves have many branches called dendrites. They come close to but never connect to other nerves. The gap between them is called a synapse. When a nerve signal comes down a dendrite, neurotransmitter chemicals are released. They float across the synapse and connect to the next nerve and a signal is produced. Thus, the next nerve in the system fires and so on and so forth. Once that’s done, the neurotransmitters that started the show are released from the affected nerve and reabsorbed into the original nerve, resetting itself.
In depression it is theorized there aren’t enough neurotransmitters to make the next nerve fire. The lack of signal moving on creates depression symptoms.
One way to make up for the shortfall is to slow down the reuptake of the neurotransmitters back into the original dendrite. It keeps the chemicals “in play” so to speak. Thus, the classes of these drugs are called reuptake inhibitors (RI). RIs have proven very effective at treating depression symptoms in patients. They have become the most prescribed medication for depression, especially as first-line treatments.
There are two classes of RIs, Selective Serotonin Reuptake Inhibitors (SSRIs) and Serotonin and Norepinephrine Reuptake Inhibitors (SNRIs). You will probably recognize many of these medications and dispense them regularly.
SSRI
SNRI
Celexa (citalopram)
Cymbalta (duloxetine)
Lexapro (escitalopram)
Effexor (venlafaxine)
Luvox (fluvoxamine)
Fetzima (levomilnacipran)
Paxil (paroxetine)
Pristiq (desvenlafaxine)
Prozac (fluoxetine)
Savella (milnacipran)
Viibryd (vilazodone)
Zoloft (sertraline)
It would be wonderful if these medications worked for everyone, but they don’t. There are side effects that can be too troublesome as with any medication. Sometimes symptoms are reduced but remain problematic. Sometimes the drug doesn’t work at all. These are cases of “treatment-resistant depression”. It is not uncommon for the doctor to try several drugs or add additional drugs to the therapy.
Other antidepressant drug classes are:
Tricyclic Antidepressants (TCAs)- These are older drugs that block the reabsorption of serotonin, norepinephrine, and acetylcholine (another neurotransmitter). You will recognize many of these drugs too.
Anafranil (clomipramine)
Elavil (amitriptyline)
Pamelor (nortriptyline)
Sinequan (doxepin)
Tofranil (imipramine)
Vivactil (protriptyline)
They are called tricyclic because they have 3 rings in their chemical structures. I know you don’t really care but I have admitted I am a chemistry nerd.
Monoamine Oxidase Inhibitors (MAOIs)- These drugs are older still. They work by stopping an enzyme that breaks down monoamines. They have proved to be troublesome to use, so you don’t see them much anymore. The only one I have dispensed in my career is Emsam (selegiline).
Atypical Antidepressants- These medications don’t really fit in other classes of drugs. Thus they are called Atypical. They can affect serotonin, norepinephrine, and dopamine.
Trazadone
Remeron (mirtazapine)
Wellbutrin (bupropion)
Combination Medication Therapy
Other classes of medication may be added to antidepressants for more effective treatments. For example mood stabilizers, antipsychotics, anti-anxiety medication, or stimulant medications.
Brain Stimulation Therapy
Electro-shock therapy in mental health has been around for a long time. Equipment and technics have improved its safety and effectiveness considerably since it was first applied. The treatment theory states that stimulating the nerves directly through electrical or magnetic charge can make them release more neurotransmitters, thus improving mood. Currently, it is most often used when other options have failed. Continued improvements in techniques and equipment are making the treatments more mainstream.
Electroconvulsive therapy (ECT) is a brief electrical stimulation of the brain while the patient is under anesthesia. Usually, ECT is applied two to three times a week for a total of six to 12 treatments. It is usually managed by a team of trained medical professionals including a psychiatrist, an anesthesiologist, and a nurse or physician assistant.
Transcranial magnetic stimulation (TMS) is a treatment where a coil is placed against your scalp. It sends brief magnetic pulses to stimulate nerve cells in your brain that are involved in mood regulation and depression. TMS is usually done in a doctor's office or clinic. It requires a series of treatment sessions to be effective. Generally, sessions are carried out daily, five times a week for four to six weeks.
How does a Doctor choose the Right Therapy?
There is no such thing as the exact right drug or therapy. What works for one person may not work for another. Even if one therapy seems to work at reducing symptoms it may not work all the time. Flare-ups are possible, or the chosen therapy may lose its effectiveness over time.
It comes down to what the doctor perceives is going on and what he chooses to do about it. There are a lot of choices for the doctor to choose from but in truth, he chooses the drug he or she is most familiar and comfortable with dispensing, most of the time. Admit it, we do the same thing. We all have our favorite tool when doing a job.
What I am trying to say is, don’t get too caught up in trying to find the exact right drug. Just go with what the doctor decides to do but keep the prescriber informed on how the therapy is working out. It becomes a matter of experience and In-home caregiving skills as a support to the patient and the doctor.
Care Home Providers and Depression
As you can see depression and its therapy are very complex. There is no way I can cover everything effectively. I was starting to feel bad about leaving so much out of this course, then I had a thought. In-Home caregivers really don’t care about the nitty-gritty details. That’s for the highly-paid Doctors and Psychiatrists to worry about. Caregivers just need to know the basics and the big things to watch out for in therapy. When it comes to the basics in care homes, you’re talking about managing the home, managing the resident, and managing the resident’s role in therapy.
Managing the Home in Depression
Managing the home in regard to depression is pretty straightforward. The main goal is to create a safe and supportive environment that is free from the stressors that can trigger or aggravate a depressive episode. It is a key component of therapy, and it is what Adult Foster Care providers do better than anyone else. You listen- when listening is needed. You don’t really care about judging the character of the resident. You can push back against the system when needed, and you take care of all the details of daily living. Boy, if I was struggling with depression that sounds like the place where I would like to be.
Managing the Resident
Managing the resident starts to get a bit more involved for the In-Home caregiver in regard to depression. It has two main aspects. Being in the position to know the resident better than other medical professionals and being the resident’s advocate.
Because you live with the patient, you are in a position to see changes in the conditions of your residents before other medical professionals. So if this is the case, how can In-home caregivers tell the difference between regular unhappiness and clinical depression? The answer is time.
In care homes, caregivers witness residents having good and bad days all the time. Usually, they come out of the funk on their own. Major depressive disorder is different in that the resident’s bad days seem to stretch out far beyond what would be considered normal for the resident. Just how long should bad days stretch out before calling the doctor? In my opinion, it is a matter of functionality. At the minimum, symptoms must last at least two weeks and must represent a change in a previous level of functioning. What functioning means is going to be different for each resident. Remember the age and gender of the resident make a difference in recognizing symptoms. Keep good records of the change in functionality and pass the notes along to the doctor.
Once you have got the therapy ball rolling it’s time to switch to being an advocate for the patient. As a patient advocate, you will have to determine if the therapy is working and if there are side effects or other issues that need to be handled. It has been my experience that side effects show up first, but it takes 4-8 weeks to see the full effect of medication. Also, side effects tend to diminish over time but not always.
If troublesome issues remain or new issues develop, skillful follow-up is a matter of asking the right questions to the right people. Don’t be afraid to ask questions like:
How come this is happening?
Could this symptom be the drug?
Is there something that could be added on to the current therapy?
Other things to consider
The primary care physician (PCP) is not the only tool in your toolbox for handling depression. Don’t forget you can ask the PCP for a referral to a psychiatrist for psychotherapy. If psychotherapy is chosen, talk to the psychiatrist to find out how you can support the therapy. You will also have to ensure that the PCP and the psychiatrist are cooperating with each other.
Exercise is proven to be an effective therapy. In care homes, the easiest exercise is regular walks or scheduled use of exercise machines. Gardening is also very therapeutic, plus the free food is always a good thing.
Managing the Drugs
I am not going into a lot of detail here. I have other courses for that. There are things in regard to depression that I think you should know about.
Typically, it takes 4-8 weeks to see the full effect of medications.
In many SSRIs there is a 2-week delayed effect. If you increase a dose, you will see the effects 2 weeks down the road. The same with missed doses or discontinued therapy.
Increased risk of suicide is a side effect. Normally the patient has no energy to follow through on thoughts of suicide. Once the medication starts to kick in, they now have the energy to act on the depression-induced thoughts. For some reason, children and teens have an increased risk of suicide within the first few weeks of therapy. Extra monitoring will be required.
Antidepressants tend to reduce the ability to feel strong emotions, including happy ones. Help the residents and members of their families recognize this fact. What appears to be a non-caring attitude may be the drugs.
In times past, stimulants or “uppers” was used as therapy for depression. Those days are long gone. They have been replaced by more effective therapy that does not have addictive side effects. In some older patients, the stigma of addictive therapy remains though. Caregivers need to keep this in mind if they see resistance to taking medication. Just ask the right questions to ascertain if this is a concern and provide the right reassurances.
Drugs, alcohol, and herbs are often used as a means to self-medicate a mental health illness. Help the resident realize this fact. Also, point out that their continued use, even occasionally, will mess up their therapy. Instead of helping it will hurt their chances to feel better.
There is emerging evidence that gut bacteria are able to affect brain function through the chemicals they release. Probiotics use (good bacteria supplements) may be effective as an add-on therapy. Adding yogurt to the diet couldn’t hurt either. Just clear it through the doctor if you intend to use it as a long-term therapy.
There is a compliance cycle issue with mental health therapy. Once the patient feels better, they think they are “cured” and try to stop their therapy. That is a Big mistake for most patients. Help the resident redefine what “cured” means. If they wish to discontinue therapy, do it in a controlled manner under the supervision of their doctor. Help the resident monitor for a relapse of symptoms.
Weight gain is often a side effect of depression drugs and can lower self-esteem.
Conclusion
Well, I hope this course on depression wasn’t too depressing. As you have noticed it is a very complicated condition. Fortunately, there are many effective therapies to choose from. The trick for an In-home caregiver is to manage the conditions of your home to be supportive and help the resident manage their therapies.
Megan Clapp. Et al. Gut Microbiota’s Effect on Mental Health: The Gut-Brain Axis. Clin. Pract. 2017, 7(4), 987; 9/15/17.https://doi.org/10.4081/cp.2017.987
Credit Hours 3 - Approximate time required: 180 min.
Educational Goal
Provide an in-depth look at the Thyroid and the hormones it produces.
Educational Objectives
Present a video about Hypothyroidism
Present a video about Hyperthyroidism
Review the anatomy, physiology, and pathophysiology of the thyroid gland
Cover the drugs used in thyroid therapy
Explain how care providers can use the materials presented to manage therapy and their resident for optimal outcomes
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.
All things Thyroid- An Advanced CE
Being required to take Continuing Education courses is never going to be anyone’s favorite activity at work. There have been many courses I was forced to take that were a complete waste of my time. I actually fell asleep at the computer during one course. We here at AFC-CE.com have tried to make the courses interesting and fun to combat that boredom. While at the same time covering topics you wanted and containing the information you can actually use in your home. There are useful topics that I would like to cover but they can be complicated and boring for all but the most diehard nerds among us. So I am going to try something new.
The topic is the Thyroid, a butterfly-shaped gland located in our throats. The hormones involved in the Thyroid are among the most important and widespread chemical cascades that you will ever come across.
As a writer I am afraid of the topic though. If I start writing about the advanced chemistry and anatomy and physiology involved, those with advanced degrees will love it. But for the rest of you, it’s going to put you to sleep. If I simplify my writing, the course will lose some of its usefulness and advanced readers will be put to sleep. So here is what I am going to do to try to please everyone.
I am going to install segments of a YouTube series, produced to tutor Physician Assistance students. The presenter is kind of nerdy himself, but in a good way. He covers the topic very well and is entertaining. I then will add my thoughts in between clips that I hope will make the information useful for In-home caregivers. Just click on the start arrow to watch the video then read my comments. I recommend that you print out the exams before you watch the course. Pause the video and write down the answers as you go. The test at the end will be easier to successfully complete that way. Fair warning. Some of this material will be pretty advanced. Too advanced for some. If this doesn’t sound like fun to you, I have plenty of other courses that you can take. If you are brave enough to proceed, I need to help you along a bit before you start the video.
Up to speed
There are a few items to cover that will help bring everyone up to speed before watching the video.
There may be terms in the video that you are unfamiliar with. For the most part, it doesn’t matter if you know all the complicated terminology. You will still be able to get the gist of that matter. You can pause or repeat the video anytime and look something up if you need to.
The Thyroid is a butterfly-shaped gland in your neck. Its primary function is to make, store and release the Thyroid hormone. The thyroid hormone can affect virtually every cell in the body that has a nucleus and does work.
The element Iodide is a chemical our bodies use to make the thyroid hormone. It is stuck onto the hormone in a particular way that forms the molecular structure. If there are 3 of them in the thyroid hormone it’s nicknamed T3, if there are four of them, T4. Both molecules are considered to be the Thyroid hormone.
There are a lot of chemicals floating around in our bodily and intracellular fluids. They usually need help crossing layers and boundaries. Like going in and out of cells.
If you see -lytic or -lysis in a word, it means to break or cut up.
Our bodies run mostly on glucose as fuel. In our cells, glucose is converted into ATP. It is a chemical that can easily release the energy our cells need to do their work.
Adipose cells are your fat storage cells
Have you got the test questions printed out? (“Hint”- You should be able to answer the first four questions.) Here is another hint there will be no question about diagnosis- you could skip those parts.
Ok, let go. Click on the start arrow.
Caregiver Notes
Is everyone still awake? For those whose eyes are glazed over go take a break and come back. Ok now? Let’s continue. Let us now go over how you can use this information in your caregiving practice. As you know Adult Foster Care providers have a different perspective on medical issues than other care professionals. We don’t decide on therapy but we do manage the resident so they can follow it. We don’t diagnose the resident, but we do monitor the resident. As an advocate when things get out of whack, we utilize any resource to the best of our ability to make the resident feel better. From this perspective let’s evaluate the video you just watched.
ManagingThyroid Issues
Management actions are broken into two duties. Managing the activities of the resident and managing therapy orders given by the doctor. The video did mention that the thyroid affects every part of our body but did not mention any lifestyle choices that affected the thyroid. That’s a good thing. There are no lifestyle effects that you have to manage. One less thing for caregivers to worry about. The therapy mentioned was also very easy to manage, for most people it will be Levothyroxine. The video didn’t give any details about the drug so I will.
Levothyroxine prescriptions are a synthetic version of T4. Brand names are Levothroid, Levoxyl, Synthroid, Tirosint, and Unithroid. Most prescriptions will be written for a generic version of the first three.
Foods can affect the absorption of levothyroxine so give the doses 30 minutes before a meal. Usually, it is given in the morning. But it doesn’t have to be as long as you are consistent with the time of administration. If dispensing the drug before meals is problematic, ask the doctor about giving it at bedtime. You can crush the medication and hide it in food, but you will have to be consistent with the amount and kind of food it is mixed in. If you have to hide it in food the doctor will have to approve it beforehand. The prescriber might order additional blood tests to see if he has to alter the dose.
Medications can also affect the absorption of levothyroxine and must be taken four hours apart. The occasional PRN dose of the drugs will probably not have any therapeutic effect. So their infrequent use is not a big issue. The drugs to watch for are:
antacids that contain aluminum or magnesium - Gaviscon, Maalox, Milk of Magnesia, Mintox, Mylanta, Pepcid Complete, and others.
If you regularly dispense any of the above you will have to consult with the doctor or pharmacist about administration times.
Levothyroxine is well tolerated. Any side effects are usually related to how normal T4 acts in the body and are dose-related. Common side effects may include:
chest pain, irregular heartbeats
shortness of breath
headache, leg cramps, muscle pain, or weakness
tremors, feeling nervous or irritable, trouble sleeping
increased appetite
feeling hot
weight loss
changes in your menstrual periods
diarrhea
skin rash, partial hair loss
Other thyroid prescriptions are Armour Thyroid (thyroid harvested from animals, usually from pigs) and Cytomel (a synthetic version of T3). Manage them just like you would levothyroxine except Cytomel does not need to be taken 30 minutes before a meal.
Monitoring-
Monitoring is broken into two activities. Monitoring for change in the resident and Monitoring for the effect of therapy. Since we just talked about the drugs let's start there.
The goal of drug therapy is to return the patient to normal functioning. Though the thyroid affects everything in the body. The video did mention certain items of physiology. When monitoring for drug effect, I recommend not getting caught up in the details but keep track of those mentioned effects as overall trends. Also, life is variable. Small changes happen every day so keep your mind on long-term monitoring, not normal short-term fluctuations.
Consistency is a key aspect of therapy. If things get out of whack, look for what has changed. Switching brands may produce lesser or greater therapeutic effects so monitor the patient more closely for a while after a change of brand. Get to know what is normal for that resident. Now that you know what to look for if you see multiple symptoms starting to occur, it’s time to contact the doctor and start asking questions.
Advocating-
Advocating for the resident is working the medical system to get what the residents need. Sometimes it feels like you’re the only one looking out for the patient. The most powerful advocating method that I know is recording measurable observations and showing the data to the doctor. Following up by asking the “Why is this happening?” questions. Better still, if you know your stuff, the “Is out of whack thyroid levels causing the issue” type of question. In a nutshell, watch for changes and ask why, if you see signs and symptoms patterns. Keep asking until you get the response you and the resident can live with. Don’t be afraid to go back to the doctor and report that his or her therapy choices don’t seem to be working as expected.
Well, that’s enough of that. Let's get on with the next video. Don’t mind that it starts out with the same info. It’s good to review the basics.
Caregiver Notes
Hyperthyroid issues-
You will have noticed that there are a lot of things that can cause too much thyroid hormone to be produced. The one that is man-made is the drugs Amiodarone and Lithium. Amiodarone is taken for cardiac and B/P issues and Lithium is for mental health issues. Both of these conditions have similar signs and symptoms to Hyperthyroidism. Someone will have to be asking the question “are these heart problems and acting abnormal behaviors issues being aggravated by Hyperthyroid conditions? It might be time for a blood test for High T4.
I would also like to point out that if there is ongoing thyroid tissue damage, there is the possibility of flipping from Hyper to Hypothyroidism. Someone will have to watch for hypothyroidism symptoms. Caregivers will see them before the doctor does so I guess that would be you.
Hyperthyroid Drugs
Propylthiouracil
Propylthiouracil can cause liver damage, especially in the first 6 months of therapy. Call the doctor right away if you notice in your resident upper stomach pain, nausea, vomiting, loss of appetite, fever, itching, tiredness, dark urine, clay-colored stools, or yellowing of your skin or eyes. Other serious side effects that must be called into the doctor are fever, chills, sore throat, mouth sores, feeling light-headed, unusual bleeding, purple or red discoloration of your skin, skin rash, skin pain or swelling, pink or dark urine, foamy urine, little or no urination, shortness of breath, or coughing up blood.
Methimazole
“Methimazole is presently the preferred one due to less severe side effects. These drugs work well to control the overactive thyroid, and do not cause permanent damage to the thyroid gland. In about 20% to 30% of patients with Graves’ disease, treatment with antithyroid drugs for a period of 12 to 18 months will result in prolonged remission of the disease.” American Thyroid Association
According to Drug.com Methimazole has many of the same side effects as propylthiouracil but has no listed liver failure warning.
Beta-blockers are a class of high-blood-pressure meds. They usually make the patient feel better within hours to days, but they do not change the high levels of thyroid hormone in the blood. These drugs may be helpful in slowing down the heart rate and reducing the symptoms of palpitations, shakes, and nervousness. If these symptoms are an issue, they are an add-on therapy you could ask the Doctor about.
For a full list of possible side effects and possible drug interaction of any drug mentioned in my CE courses, see the drug insert that comes with the prescription.
Thyroid function Tests were mentioned in both videos. Caregivers should know that estrogens and Biotin can interfere with these test results.
Conclusion
Being such a relatively small organ the Thyroid has a big impact. I hope you enjoyed the way I covered some of the basic concepts. There was a lot more I could have covered but I have to cut it off at 3 hours’ worth of materials. I hope you can use the information to better manage, monitor, and advocate for those in your care.
Credit Hours 3 - Approximate time required: 180 min.
Educational Goal
Teach how to make the new resident move in process easier with less problems.
Educational Objectives
Review the actions to take before the new resident moves in.
Make suggestions for moving in day.
Provide expectations and recommendations for after the new residents moves in.
Teach about 3 different care perspectives
Provide additional helpful hints.
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.
Smoothing Out the Moving In Process
Very few people like the labor involved in moving to a new home. I can genuinely say that my wife dislikes the moving process so much that it has almost becomes a phobia. Who’s to blame her for her feelings of dread and concern. There is the exhausting and confusing work of sorting, packing, and physically moving. There’s the emotional trauma of leaving the comfortable behind, coupled with the feeling of loss of saying goodbye and the fear of heading for an uncertain future. There is also the constant worry of hundreds of questions that do not have immediate answers.
The same feelings, worries, and concerns are experienced by each new resident that moves into your home. In addition, there may be feelings of abandonment by the resident, feelings of guilt felt by family members, worry over finances, and the bewilderment of trying to adjust to a whole new lifestyle circumstance. Now add to all of the above with the life alterations caused by medical concerns and it’s easy to understand that the moving-in process can be a very traumatic experience.
But what about me and my traumas, I hear you say. Yes, caregivers also face extra work, worry, and concerns. You are the one who has to take a traumatized patient and integrate them into your life. Unlike other medical professionals, you don’t get to leave when your shift is over. You have to stick around and endure until the trial is over. As a caregiver, some of my worse days in the profession were all related to an ill-prepared and uncooperative new move-in resident. But as the saying goes “Trials are great teachers - if you are paying attention” The following are some of the actions to take that I and other caregivers have learned in the school of hard knocks. Hopefully they that will help you smooth out what can be a very bumpy road.
Before they move in
Making the transition to your home smooth starts way before they move into your home. To prepare the potential new resident you have to remove doubts, answers questions, and assuage fears. You will have to show that you will respect the family and the resident.
You will also have to engage in a little theatrics to make your home appear desirable. The goal is to make the patient (and their family) want to move in. Remember that you are competing with other institutions and the comforts and familiarity of their own home.
1. Remove doubt by being a medical professional.
You are more than a bed and breakfast or a glorified babysitter. You are “THE” In-Home care expert. You must learn how to convey to the patient and their family that you are an expert medical professional. You have the skills to expertly handle any medical considerations that may arise. This will instill confidence that the new resident is making the right choice in moving into your home. Remember that is the main reason why they are looking at your home. Someone has admitted that the patient cannot handle the medical concerns themselves and is looking for help.
You do not have to be a therapeutic expert on anything (though any medical credentials you have can be presented as a bonus feature of choosing your home). You do have to be able to convey that you are a patient advocate expert. Show that you know how to work seamlessly with any medical professional that is or will ever be required in medical care.
Show them your record systems to provide proof of how you communicate critical information to other medical professionals, manage medical and medications monitoring, and manage future medical requirements like doctor appointments.
Tell them specific examples of business procedures that you have in place that ensure a smooth-running operation. For example, medical records that are sent along with the patient to doctor’s offices and how you follow up afterward the visit.
By conveying that you are an expert patient advocate you will provide ease of mind that medical concerns will be taken care of. Use the phrase One less thing to worry about, I’ll take care of that for you. Emphasize that you are on their side and will do battle for them if needed. It’s reassuring to have powerful friends that the resident and the family can count on.
2. Remove fear and concern through interaction.
Tell them stories of how you handled difficult situations and or difficult medical professionals that resulted in a positive outcome for the resident.
Ask the family what questions they have but ask the resident what fears they have about moving. Write down the question before answering to show that you are listening and showing respect. Including the resident in this way helps them on several levels
Gets the resident to emotionally by into the thought of moving into your home as you address their fears.
Gives them a semblance of control and respect when circumstances are taking away control and respect.
It helps the family know the reasons behind any resistance to moving.
It also gives you a window about future efforts that may be required of you.
Steer the conversation away from the “you need help” phrase. No one likes to be reminded that they have failed at something. Rephrase the concept by telling them they are smart in choosing a place that has more resources that they can take advantage of to improve their living standard. “Haven’t you dreamed of having a cook and house servants to make your life easier” is an excellent joke at this time, if done right.
Invite the resident to a free meal. Give them a menu and make a lunch or dinner appointment. Offer to pick them up and drop them off afterward. This will give you a peek at their current living conditions and show that you are willing to go out of your way for them. This will also help them get used to coming to your home. Sort of a trial run so to speak.
3. Make them feel comfortable by interacting with their senses
You would be surprised at how senses affect the way we think and determine the choice we make.
When the potential resident makes their first visit, make your residence smell like home. Make a treat and serve it to everyone fresh. You can enhance the aroma and entice their tastebuds by boiling cinnamon on the stove.
In general, offer cookies for kids (mental kids too) cake for ladies, and pie for men.
Make sure the curtains are open, letting in the warm sunshine to brighten the place. Don’t forget opening the curtains in any bedrooms that you show.
Enhance colors with table centerpieces of flowers or holiday decorations.
Spiff up your current residents. Put your best foot forward. No food-stained shirts, comb everyone’s hair and eliminate odors.
4. Give the potential new resident a voice
Moving to your home will have the potential of feeling like they’re losing their freedom and control over their life. Involve them in the conversation so they can claim ownership of the move-in decision.
5. Take advantage of your strengths
Take advantage of being an actual home and not a cold institution. Point out that they will not be alone anymore. They will have people like them to interact with. Also, remind them that someone will constantly be on the lookout for them.
Take advantage that you do not cost as much as a larger institution. People like to save money.
Take advantage of the fact that every meal served is a home-cooked meal, not bulk cafeteria food.
Take advantage of the fact that you will be taking care of all the chores that they hated to do in their own home.
The goal of all the above is to make the new resident want to move in. If they are looking forward to the comforts, ease, and security of living with you, they will be spending less time looking for the misery of giving up their home and independence. Prepping the patient in this way will make a smoother transition into your home.
After the family has chosen your home to live in, if you sense the new resident is still resistant to the move, it would be advantageous to have them visit one more time. Or you could visit them in their home. In this visit, start gathering information from the resident and family about the patient. Act as if they are already going to move in and you are just writing down the information that will make the transition smoother. Your questions should include:
Food likes and dislikes
Favorite activities
Favorite shows
A complete as possible medical history/record
A list of all doctors, dentists, and therapists they are seeing.
Allergies
Find out who the resident listens to and usually obeys.
What personal items do they want to bring with them?
List again the fears the resident has about the move. It doesn’t matter if it is the same list as before. People forget previous conversations or maybe your first answer was not good enough. This time, acknowledge their fears and say that what they are feeling is a normal reaction to the unknown. Add to the conversation that you have plenty of experience in solving their concerns and you will be there to help them with any problem that may occur. The goal is to start having them rely upon you to solve their problems. Remember the phrases and techniques that seem to work so that you can use them in the future.
While they move in
Moving day, from my perspective it isn’t all that difficult. Just move the stuff in, arrange it properly and make the new resident feel welcome. From the family and the patient’s perspective, it can be a nightmare. Emotions can run very high, and the sense of loss and guilt can be keenly felt. This is where you can step in and provide the physical and emotional support that can make all the difference.
What to bring.
Most of your new residents have never made a move like this before. A move where they are transferring the resident and not the possessions. Providing some guidance in a form of a list of items to bring will ease things considerably. On that list emphasize the goal will be to bring items that will enhance familiarity and provide a sense of continuity.
For example
List of what to bring when you move in
(please remember to only select items that will bring comfort and provide familiarity to their new surroundings)
o Pictures
o Knick knacks
o Pillows,
o Comforters/quilts if they have a special connection to them,
o Toiletries (electric razors only, toothbrushes, combs and brushes, perfumes, dental trays,)
o Stationary, puzzles and other such favorite past-times
o Music
o Medical devices and all associated equipment and supplies
o Clothes
Label everything including clothes.
This will help you keep things straight and provide boundaries between residents. Developmentally disabled and dementia patients are not as aware of the concept of personal property. Labeling will help you track down items that go missing, which always happen. It’s funny how a permanent marker can help you avoid conflict.
Large items.
De-emphasize household goods and furniture. They will just complicate the move-in process and add stress and weariness when it’s not needed. After all, you are a care home and not a storage facility. Sometimes though it can bring comfort to have a few big items around. I remember bringing in a baby grand piano into our home once. Use your experience and people observation skills on what big items will help the resident adjust quicker and what will be just a lot of unnecessary confusion causing extra work.
Bedrooms
In my experience bedroom furniture is an exception to the large item rule. Bedrooms are like a pseudo-apartment. It is the haven they can escape to when they want to be alone. It is also the environment where their brain is the most tired and prone to confusion. Either in the low light of the middle of the night or upon getting up before they are fully awake. Having a lot of familiar items around helps relieve confusion considerably. Also, you sleep better on your own mattress and pillow.
Arrange and decorate with purpose. Eliminate trip hazards and make access to clothes and the bathroom a priority. It will have the added benefit of making your daily chores easier. Add bright and positive colors with pictures or flower arrangements. Put a personalized wreath or other personal items on the door. It labels the room “Home” and helps with navigation in the early days after the move-in.
An above and beyond idea that has several benefits is involving the new resident in making the door wreath or plaque. Have them choose the personal items to include and or sign their name. Take a picture and add it to the display. Their involvement helps them feel in control and labels the place “Mine”. It also gives them something to show off to visitors.
Dementia.
Take time to train the family before moving day about the special care requirements of dementia and the developmentally disabled. When there is dementia or other limited mental acuity issues the family should do most of the selecting and packing of items. Leaving all the decisions to these kinds of patients can add too much stress and lead to serious confusion and lashing out in anger. Also, be cautious with discussions about moving before moving day. The more limited the mental capacity the easier it is to get them wound up and worried (anticipation anxiety).
It will be a balancing act between including the patient in the decision process to garner cooperation and pushing them over the edge. When in doubt go slow, take time to pack over several days, and move when they are at their mental best. Reduce the surprise factor as much as possible. Another suggestion is to take the patient on an outing and while they are gone move all the items. In these types of moves be ready with explanation talks with the new move-in.
One trick I heard of is giving a baby doll to take care of. The doll can become real in a sense and have a great calming effect. Some memory care units even have baby stations.
“While the baby doll approach isn’t limited to only women, men might respond to tools, stuffed animals, woodworking, and other crafts. The theme here is that when facilities figure out what your loved one was interested in as children, they can help recreate aspects of those interests. You might have key insights that can lead to a breakthrough.” – Pam Silverberg
The best time to schedule the move is mid-morning when they are rested and fully alert, or Mid-afternoon. Suggest a time when all your house chores are done so that there will be less commotion and you can fully focus on the new resident. A calm environment will be easier for patients with dementia.
Medications, medical devices, and therapies.
If there is no primary care physician get one before you allow anyone to move into your home. Because the most important conflict-relieving thing that you can do is to get approval in writing from the primary care physician on all medications and therapies. Do it before the resident moves in or at least as soon as possible thereafter. Doing this in a timely fashion will allow you to use the primary care physician as a shield to deflect most arguments with the new resident about medical concerns. They will be less able to argue with you about such matters because you are just following the doctor’s orders.
If difficulties continue you can still deflect the issue by saying something like, “I understand the confusion, with the move and all it’s easy to see how the ball was dropped. Let’s make an appointment with the doctor to get these things straightened out.” If they still refuse to cooperate, they still have a right to refuse. Record the refusal in the MARS and send all the details to the doctor. Let the primary care physician deal with the problem, that is what he or she gets paid for.
You might be able to sidetrack the whole affair with some astute questioning about why they are refusing. It might be as simple as they are tired and don’t want to deal with any more changes. They may also have a misunderstanding of what the medication does or a fear of what will happen if they have a change in their medication routine. Arguments such as these can be handled by saying that you are on their side and will monitor the situation closely to prevent problems. You can also say “I will pass on your concerns to the doctor at my earliest convenience and will help straighten out the issue.
I suggest the most efficient way to handle medications is either to visit the home or have someone responsible go through the house and record everything they find. Remember to include OTC, herbal remedies, and expired medications.
Make a list of all medications found and send it to the primary care physician. Include the prescribers name, strength of the medication, the instructions, and date of expiration.
Do not assume the primary care physician knows what is being taken. All too often, nobody told the doctor about medications from other prescribers, or the patient has kept taking discontinued medications for various reasons.
Remember to follow up with the doctor on what to keep and what to throw away.
Get prescriptions for all OTC meds.
Make an updated list of meds and get into the MARS.
Work with your primary pharmacy to transfer all approved prescriptions and fill new otc prescriptions.
Don’t forget to give insurance and allergies information to your pharmacist.
Be aware that the medication may look different from what the patient is used to. Different pharmacies use different generic brands. You can resolve such issues by reading to the patient the pill description off the prescription label, auxiliary stickers on the bottle, or information sheet that comes with every prescription.
If you can accomplish these medication-related tasks before the new resident moves in that will make things a lot easier for you.
Little courtesies.
It is easy to focus on the physical aspects of the move and forget the emotional needs of the new resident on moving day. Keep your eye on the patient and watch for body language and verbal clues for warning signs of too much stress. Stop every now and then to just talk to the new move-in and or their family. Kind of like when a waiter checks in at the table at a restaurant.
Other little courtesies are:
Prepare a favorite snack or meal on the first day of arrival. Comfort food takes on a whole new meaning on moving day.
Give a move-in day present.
Give contact information to the family on premium giveaway items, like pens, paper pads, calendar, frig magnet, etc.
Have their favorite music playing in the background. Don’t underestimate the comfort power of a favorite tune.
After the bedroom is set up, see if they would like to take a nap.
Be prepared to hear complaints.
Make sure you are really hearing the resident’s complaints. Just dismissing their validity can lead to even bigger issues later on. Do not view complaints as a negative. View them instead as a call for help. Be patient and be ready to explain what is happening over and over again. Often what is really wanted is just a reassurance that everything will be okay. Point out how wise they have been in choosing a place that will improve their lives, then list the features of your home.
There are those who need to work things out verbally and complaints are just their way of adjusting. Fear of the unknown also drives negativity. Empathy statements are just the ticket in these cases. For example, “Moving is such a pain, right? Don’t worry, you’ve survived far worse things in your life.”
Remain positive and upbeat regardless of what happens or what is said. The new move-in will most likely reflect your positivity back to you. If you are anxious or fretting, they will reflect that back to you. Pass on the same advice to the family members involved in the move.
The family.
Be aware that the move may be harder on the family than the resident. Their feelings of guilt and anxiety are poison to the environment on moving day. Watch for the warning signs and be prepared to help.
Keep them engaged or occupied with tasks.
Acknowledge their fears and show empathy.
Remind them they are doing this to give a better quality of life for their loved ones.
Do not be afraid to politely remove them from the situation. For example, “I have things handled here, why don’t you take your loved one for a walk so they can become familiar with the neighborhood. Be back in about 15 minutes”
After they move in
The transition process continues long after move-in day. The ability of the new resident to cope with the change will vary widely. It depends on what life skills they have developed, what medical conditions handicap their efforts, and what support they get from their family. It can take new residents up to 3-6 months to finally call your home their home.
Do not make the caregiving mistake in thinking this settling-in process will happen quickly or automatically. Developmentally disabled residents will have a reduced ability to understand what is going on. Mental Health patients’ minds will be tainted by their conditions and geriatric residents have physically lost some of their ability to cope with change due to the aging process.
It is critical to understand that these new residents are patients that need your caregiving skills to adjust to their new surroundings. It will take much more than being patient. Caregivers will need to take an active role in assessing where the difficulties lay and overcoming any conditions that may prevent a smooth transition.
Unfortunately, I know of no “one size fits all” program or set of procedures that will work in all care homes. There is no large college or government department studying how to best run a care home to optimize the assimilation of new residents. The only school that I know of that will tell you what will work for you is the school of hard knocks. The following material is what the school of hard knocks taught me. Use this material with an open mind and a grain of salt. I hope you will find it useful and effective.
Care Philosophy- The Benevolent Dictator
This is not” Do what I say because I’m in charge”, which rarely works. Believe me, I tried that over and over with the same lousy results. It is more,” Do what I say because I know best” This will work on the developmentally disabled, autistic, and the shy or timid patient. You can tell which patient to use this care philosophy on because they will be
Constantly asking for directions on what to do next.
Blank or confused in facial appearance or body language. The absence of reaction is actually the resident quietly waiting for the next set of instructions.
Constantly worrying that they are doing something wrong.
When you observe these tendencies be ready to step in with an organized program and stick with it until it becomes a habit. This approach will work better if you apply it as a teacher, not a prison warden. Compassionate and patient consistency will be the key to a smooth and speedy assimilation into your home’s routines. If difficulties arise, first ask yourself, “what don’t they understand”. You can also garner cooperation by allowing them some input on when and how things are down. Some suggested tools to use are:
Have orientation sessions that instruct how to fit into your home’s routine.
Written step-by-step procedures that the resident can use as a reference. You can post them in their room or laminate pocket-sized versions for personal use.
Picture Flashcards that show what to do next. You can make your own or do an internet search for free downloads. Use the search phrase “activities of daily living flashcards” to get started. You will have to worry about being age and ability appropriate in their use.
Apply labels such as drawer contents, door labels, and table setting assignments.
Care Philosophy- The Compassionate Manipulator
This is a care philosophy whose goal is to work with perceptions and influencers to maneuver a patient into choosing to cooperate by themselves. This works well for those whose sense of reality is impaired such as in dementia.
In dementia, the patient’s ability to perceive their environment has been physically impaired. They do not act the way you want them to because their reality is different than yours. It takes a great deal of effort to argue them back to your reality. It is much easier to match their reality and then reason with them.
I heard a story that is a perfect example of this. An Alzheimer's patient wandered out of the facility where he was staying. The staff asked a visiting barber to help in the search for him. The lady barber found him wandering down the street. She asked him what he was doing and he said he had to go to work. She entered into his reality and said “Look at you, you’re not ready for work, you look a mess. Let me help you back to your room where I’ll help you spiff up. He voluntarily followed the barber back to the facility. Everything was going well until they entered the facility where the staff practically tackled the patient and dragged him back to his room. Which approach do you think was easier and more successful?
Some suggested care techniques are:
Appeal to trusted authority- Until you earn their trust, they will not readily follow your instructions. So, find out who they do trust and phrase the instructions as if they came from them. Also, have that trusted authority endorse you often.
Divert attention- Do not confront the issue head-on, first get them to think of something else and then ease into the instruction from the side. An example is if they are wandering around trying to find non-existent stairs say “Okay, let’s look past the kitchen”. Then offer them a snack. When they finish the snack and say, “I just love snacks don’t you? Now, what were we doing? Oh yes, I remember now. We were heading to (fill in instruction)
Short-term memory loss- Take advantage of short-term memory loss to make it appear that have already agreed with the instruction. For example-
This is what you always have done, it must have just slipped your mind. Do you really want to change now?
You told me to remind you of (instruction) if ever you forgot again. I’m just doing what you told me to do.
Control the environment to reduce confusion. Too much input overloads a compromised brain leading to confused behavior. Limit choice selection, make the choice for them, reduce noise, reduce commotion, etc.
Care Philosophy- Root of the Problem
I have done it myself. You’re involved in getting the morning chores done and a problem arises. You’re busy so you make a snap judgment of what the problem is so you can speedily resolve the issue. But you guessed wrong, and the problem escalates. The keyword is guessed. I wonder how many problems we escalate by guessing at the solution before we understand what is causing the problem behavior. Care homes do have their busy moments. But in reality, your day is not that filled up. There is almost always extra time in the schedule to find the root cause of an issue. Take the time to ask the right questions, really observe behaviors, and search for the root cause of the problem.
Case in point, a normally rationally acting elderly lady would sometimes get very confused and try to enter into several neighborhood homes. After really looking at the situation it turns out that she would get confused only after taking multiple prn medications. When taken together, they caused dementia-like behavior. The answer was not more drugs to control behavior, but fewer drugs.
Here are some caregiver tools that can help you get to the root cause of a problem.
Look for chemical crutches that only mask the root cause of an issue
I would venture to say that the vast majority of new move-ins are on too many drugs that rely on relieving symptoms to cure a problem. I call them chemical crutches. It is understandable that this happens. A patient develops a health issue and they go to the doctor's office seeking a solution. The busy doctor usually responses by prescribing a drug to control the symptoms of the problem. The symptoms are resolved so the patient thinks they are “cured” and stops taking the med. But the underlying cause remains so the problem returns. The caring family notices another occurrence of the problem so they, in turn, insist on getting another pill from the doctor to “cure” the problem. Then the patient goes to the ER and obtains another medication, etc, etc, etc. This phenomenon is called medication overload and it is a real epidemic problem today.
I suggest that when a new resident moves in, you review their med list with the purpose of getting rid of unnecessary drugs. In-Home caregivers are in the perfect position to reduce medication overload. You live with the patient and have the time and opportunity to control problems without having to rely on chemical crutches type solutions. Since you are working on the underlying cause of the issue it tends to stay under control. In addition, since there are fewer drugs used, there are fewer drug-related problems that crop up. That means fewer side effects, and fewer overly medicated patients to deal with. As a bonus, there is less MARS charting to do. We all want that.
Look for alternative explanations of what is going on
Take the time to think about alternate explanations before responding to issues. Like Sherlock Holmes, do not jump to conclusions but use all your senses to search for underlying causes.
I remember an elderly gentleman who started to have behavioral problems. I asked him some questions and he would not cooperate. I paused and thought, “what is the root problem?” I then noticed that one of his pupils was larger than the other. He was not acting up. He was having a stroke.
Use empathy to address the emotional elements of an issue
Humans are not rational creatures. We tend to respond to issues emotionally. We use anger or sadness as emotional tools to get other people’s attention. The emotional signaling will continue until they are acknowledged, and appropriate action is given. The use of empathy is an effective way of acknowledging the emotions the resident is feeling. It tells the patient that we understand why they are emotional and are here to help. When we validate the need for the emotion then there is no need for it to continue and the emotional behavior subsides.
Just to be clear, the definition of empathy is the capacity to understand or feel what another person is experiencing from within their frame of reference, that is, the capacity to place oneself in another's position. Acknowledging feelings is like empathy in work clothes. I found an example of how a dementia care specialist used empathy to deal with a dad who was having difficulty transitioning to a memory care facility.
“This is what I do instead: I listen. I listen to every last bit of it. True, it’s easier for me because your dad isn’t pushing my buttons. Still, I listen. And I empathize and validate. Instead of trying to convince your parent how great it’s going to be, I listen and then I tell him I can absolutely see why he’s so upset. I’m certain I’d be upset too! I hate the whole deal for him. I reassure him he never, ever has to like it. The End. No arguing.”
With the emotions under control, you can now deal with the real problem. What care philosophy works the best is case-specific. Practice at all three so you can be skilled in any situation. The harder you work at this the easier your job will get, and we all like easy.
Visits from Family and Friends
Visits from family and friends is an important resource that caregivers can utilize to make the new resident feel more content in their new surroundings.
Visits can fight depression and reduce feelings of abandonment.
They are opportunities to build trust as families endorse you as an expert.
Praise from family can build pride in accomplishments in the resident.
Visits are opportunities to blow off the steam of frustrations and work out their feelings with someone who cares.
Visits can divert attention away from complaints.
But be careful, visits are also a double-edged sword that can cut both ways. They can add to the confusion, create tension and emphasize misery. Pay attention to how the patient reacts before, during, and after the visit to determine if the visits are helping or hurting the settling-in process.
To minimize negative outcomes, train family members how to effectively visit to help with the transition. Depending on the amount of dementia forgetfulness or other mental handicaps, encourage short but frequent visits. Try to discourage outings until after they have more or less become comfortable with your home. Offer in-home activities to make the visits more meaningful (host a tea party or provide the materials to create a photo album).
Utilize technology. Emails, Texting, telephone calls, video chats, Zoom meetings, and skype chats can all be used instead of in-person visits to increase visits or control interactions that cause difficulties. Finally, do not overly rely on the family visits to solve problems. It makes you look like a poor caregiver in the eyes of the family.
Other Helpful Hints
Routines build habits and habits create a familiarity that turns a house into a home
A photo collage board or display of new and old pictures creates a bridge between old and new living arrangements.
Create an activity box filled with elements of old hobbies so that their favorite interests can continue or be rekindled.
Provide materials or act as a scribe to encourage writing letters or greeting cards to loved ones.
Provide kid-friendly activities for visiting family members to reduce the trouble board kids can create.
Do not prejudge negativity as bad. Instead, see it as a request for attention. Listen to the emotions behind the words. Is it anger or fear that drives the complaint? Pay particular attention to non-verbal cues, like body language, facial expressions, posture, and gestures. They can help you determine the seriousness of negative comments.
Encourage friends and family to bring activities with them to make the visit more enjoyable.
Always have an activity ready that can be used as a diversion to take the mind of the resident away from troubling behavior. Walks, magazines, treats, music, games, puzzles, computer games, and cards can all be used to divert attention.
Be prepared for bad days and expect setbacks. They are just part of the caregiving profession. Remain positive, be in control and act proactively and bad days will pass. Be assured that they always do.
Conclusion
Moving in a new resident is a lot of work for the caregiver, patient, and their family. It requires an adjustment to a new life circumstance that may or may not go smoothly. In-home caregivers should not assume that the needed adjustments will happen automatically. They should be prepared to take an active role in the transition process. Caregivers should plan ahead to ensure that the training, resources, and materials are there when they are needed to handle problems and speed up the transition process.
Credit Hours 1 - Approximate time required: 60 min.
Educational Goal
Teach about Antiplatelet and Anticoagulant therapies.
Educational Objectives
Provide a brief overview of the blood clotting process.
List symptoms of internal bleeding
Teach about antiplatelet medications.
Teach about anticoagulant medications.
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.
Caregiving and Blood Thinners
When I was operating my own adult foster care homes there was one medication that constantly resulted in uncomfortable questions for county health officials, Warfarin (Coumadin). Warfarin is comely known as a blood thinner, we called it the bruiser medication. Blood thinners reduce the chances of dangerous internal blood clots that can cause a lot of damage. They also make it easier for minor cuts and abrasions to bleed profusely on the inside and outside. If an elderly resident bumped into the door a little too hard, a rather large bruise would inevitably form. It made it look like we took a bat and beat up the resident. Not a good look for a care home. It always resulted in abuse questions. Blood thinners are a high maintenance drug class that requires the In-Home caregiver to manage the patient and medication- carefully.
What are blood thinners?
I don’t know how everyday names for drug classes get started. They are often just flat-out wrong. Blood thinners don’t actually thin the blood. They are medications that make it harder for the body to form blood clots (coagulation). There are two types of so-called blood thinners that work in different ways to prevent dangerous emboli from forming. They are antiplatelet and anticoagulant therapies.
Coagulation, or the blood clotting process
To help you understand blood thinners, let’s review how blood clots. The clot formation process is surprisingly complex. It involves multiple cells and blood factors that are constantly flowing through the bloodstream. When a blood vessel is damaged blood platelets are activated. They stick together at the site of the damage and form a weak plug. The plug is strengthened by clotting factors also flowing in the blood. Fibrin a special clotting factor that comes together and forms a mesh of fibers. The fibers act like the glue that holds the platelets, red and white blood cells, and other clotting proteins together and a clot is formed.
Blood platelets are fragments of white blood cells and they flow through our blood. Having the shape of a plate they are designed to stick together at the site of cell damage in response to activating chemical signals. After they are activated, they change shape by growing tendrils that help them form a plug. After they stick together, other reactions occur, and a clot forms. The antiplatelet medication interferes with the chemical cascade of reactions between platelets, thus inhibiting a clot from forming. In laymen's terms, it makes the platelets less sticky.
Common Antiplatelet medications are
Aspirin
Clopidogrel (Plavix)
Dipyridamole
Ticlopidine (Ticlid)
Anticoagulant
Anticoagulant medications target the clotting factors, proteins made in the liver that are essential in forming a clot. These clotting factors cannot function without Vitamin K. Anticoagulant medication such as warfarin and heparin compete with Vitamin K and slow down the clotting process. Anticoagulants are more powerful at sopping clot formation than antiplatelet therapy.
Common Anticoagulation medications are
Warfarin (Coumadin ,Jantoven)
Heparins (Lovenox, Fragmin)
Dabigatran (Pradaxa)
Rivaroxaban (Xarelto)
Apixaban (Eliquis)
Why take blood thinners?
The body puts a lot of effort into blood clotting to seal up damaged blood vessels. Why would you want to prevent that from happening? Not all blot clots are beneficial. There are times when they form in the wrong places. As a result and an embolus is formed that blocks off blood flow in a blood vessel. If that clot forms in the lungs a pulmonary embolism is formed. If it forms in the brain a stroke happens. If it forms in the heart muscle a heart attack occurs. All are life-threatening. In addition, clots can form in the veins of our extremities and a potentially painful deep vein thrombosis (DVT) occurs. Unwanted clotting can also occur with the irregular heart rhythms of atrial fibrillation (Afib), after surgeries, or when medical devices are implanted. Some of these clots can break away and travel to the lungs, heart, or brain. To prevent unwanted coagulation in these and other at-risk groups, doctors will prescribe blood thinners. Unfortunately for these patients they now have to worry about normal cuts and bruises. For patients on long-term therapy (even low-dose aspirin), it becomes a balancing act between wanted and unwanted blood clotting. Caregivers find themselves with the extra work of monitoring the blood-thinning therapy and managing lifestyles to reduce and prevent harm.
Caregiving and blood thinners
In-home caregivers are in the powerful position of being with the patient more than any other medical care provider. They have more influence on the day-to-day activities of the patient than even the doctor. As such they are in the best position to ensure patient adherence to therapy (both drug and lifestyle alterations) and monitor for side effects.
Sometimes though our medical system treats In-home caregivers as if they were glorified babysitters or are just invisible to prescribers. There are those who seem to think that In-Home caregivers are unwilling or unable to follow therapeutic instructions. Regardless of the perception of others, In-Home caregivers have got to step up and insert themselves in such a way that important instructions are communicated to them. If you don’t the doctor, pharmacist, nurse, or therapist will give the information to the patient or whoever drove them to the medical appointment. They will assume that the patient will pass on the information and instructions to the caregiver correctly. Yeah right, like that is one activity that will never go astray.
Regarding the above, I was going to list all the lifestyle changes that will be required by the various blood thinner therapies but realized that would be a lengthy list indeed. It would be more advantageous for In-home caregivers to get the specific requirement of therapy straight from the prescriber.
In general, those instructions would include.
No alcohol
No smoking
Don’t start new medications, herbals, or supplements without talking to your healthcare provider. That especially includes NSAIDs and aspirin which have anti-blood-clotting qualities. You might have to switch to Acetaminophen (Tylenol, APAP) for “as needed” pain therapy.
Never double a dose because you missed a dose.
Tell anyone giving the patient medical or dental care that they are on blood thinners.
Take blood thinners exactly as prescribed.
Monitor for signs of bruising or bleeding even in normal activities like brushing or flossing teeth.
Control strenuous activities but retain an active lifestyle.
Follow dietary guidelines that are laid out in blood thinner therapy.
The Signs and Symptoms of Bleeding
Once the therapy has been established and the correct lifestyle choices have been received the next thing for In-Home caregivers is to monitor the patient for the signs and symptoms of bleeding. There is always the chance of the current medication dose working too good, the patient springs a leak through accident, injury or that something (food, drug, or herb) has added to the blood-thinning effects of the medication.
Watch for
Severe bleeding, including heavier than normal menstrual bleeding
Pink, red, or brown urine
Black or bloody stool
Severe headache or stomach pain
Joint pain, discomfort, or swelling, especially after an injury
Vomiting of blood or material that looks like coffee grounds
Coughing up blood
Bruising that develops without an injury
Dizziness or weakness
Vision changes
Head injury, even if you're not bleeding
Bleeding from the gums after brushing the teeth
Diarrhea, vomiting, or inability to eat for more than 24 hours
If any of the above occur, call the doctor. In the case of severe bleeding, call 911 and tell them that blood thinners are involved.
Note to caregivers
If despite your best efforts significant bruising occurs, I would suggest that you let any visiting medical professional, government regulator, family member, or another significant visitor that the bruises were from blood thinner therapy. Do it in such a way that it does not appear that you are covering up abusive caregiving. And of course, notify the doctor. The therapy might have to be adjusted.
From Aspirin to Warfarin- all the details
The following are some specific instructions and details that I think are important for caregivers to know.
Low dose aspirin-
81 mg therapy is roughly about ¼ of a regular strength aspirin. To save money you could break up a regular aspirin, but I would not recommend it. It’s time-consuming and messy. It would also require a new prescription from the doctor to do so.
There is a possible rebound effect if therapy is stopped. That means there is an increased chance of adverse events occurring. Counsel with the doctor about how to taper off if therapy is temporarily halted or discontinued.
If there is a constant upset stomach, counsel with the doctor about switching to enteric-coated aspirin.
Along with the regular side effects, aspirin can cause tinnitus or ringing in the ears. Periodically question the patient about their hearing.
Antiplatelet medications-
Gastrointestinal bleeding is the most common adverse event associated with any antiplatelet agent. If there are signs of blood in the stools suspect a Peptic ulcer and counsel with the doctor about such. The most prevalent sign of a peptic ulcer is a painful stomach. Remember you don’t have to diagnose a condition you just have to suspect it and bring it to the doctor’s attention.
Several medications in this group may cause hypotension. Watch for dizziness upon standing or sitting up.
Sudden stopping of some of these medications may increase the risk of heart attacks and strokes. If a patient wants to stop, find out why. If the patient is serious about stopping completely, notify the doctor of the patient’s desires and tell the patient that sudden stopping may cause serious problems. Missing a dose here or there is not a big problem, just as long as the refusal is documented and doesn’t happen too often.
Anticoagulant medications
Dabigatran (Pradaxa), Divaroxaban (Xarelto), and Apixaban (Eliquis) all are newer medications that have less interaction with food and drugs. As a result, they do not require frequent blood tests to adjust the dose. But they are more expensive, and the blood-thinning effect does not last as long. They may take twice a day dosing and refusing the medication may have more health risks than other blood-thinning drugs.
Headaches, dizziness, and bowel or bladder dysfunction may occur in the elderly
Cold intolerance may increase.
Heparin takes a lot of skill to administer and monitor. They are usually reserved for hospital or advanced nursing facilities. In-home caregivers most likely will not have to deal with these meds. If you do have to deal with them, get plenty of training and nursing delegation even if you are just monitoring the patient.
Warfarin
Warfarin is a vitamin K antagonist. It blocks the action of vitamin K in the liver thus preventing the production of clotting factors. It has been prescribed since the 1960s, so it has been approved for several disease conditions. It is also inexpensive, so you are likely to see it use in your home.
Unfortunately, many things can interfere with warfarin’s function in the body. Drugs, food, herbs, and supplements can cause a change in warfarin’s effect, both increasing and decreasing. Due to this variability, a periodic blood test will be required called the International Normalized Ratio (INR) to ensure warfarin’s safe use. It measures the time it takes for blood to clot or the prothrombin time, or just protime (PT). At first, the tests will be frequent, daily, or multiple times in a week. If the INR is too low, blood clots will not be prevented, but if the INR is too high, there is an increased risk of bleeding. Once therapy has been normalized and the variabilities of the patient’s life controlled, the test will most likely become monthly or longer.
Note to caregivers
There may be times when the dose of warfarin will change a lot. Normally you throw away the old medication when a dose is changed. That is not necessarily the case in warfarin. You can also crush and cut warfarin tablets. You might be able to take advantage of ½ tablets in dosage changes to use up old meds and save money. Get permission from the doctor before crushing or breaking tabs
Controlling variability is where the In-Home caregiver comes into play. It is very important for conditions for the patient to remain the same. Follow medication orders religiously, strictly control PRN (as needed) medications and keep meticulous MARS records and be very aware of foods that affect vitamin K levels and interfere with warfarin’s metabolism.
If there is a sudden change in INR or it fluctuates ask the pharmacist to review the drug list and prn logs to see if medications are causing the change.
Common drugs that can interact with warfarin include:
Aspirin or aspirin-containing products
Acetaminophen (Tylenol, others) or acetaminophen-containing products
Antacids or laxatives
Many antibiotics
Antifungal medications, such as fluconazole (Diflucan)
Cold or allergy medicines
Nsaids (Ibuprofen or naproxen sodium)
Medications that treat abnormal heart rhythms, such as amiodarone (Pacerone, Nexterone)
Sleeping pills
Certain medicines used to treat convulsions
Corticosteroids or other cortisone-like medicines
Common supplements that can interact with warfarin include:
Coenzyme Q10 (ubiquinone)
Dong Quai
Garlic
Ginkgo biloba
Ginseng
Green tea
St. John's wort
Vitamin E
Common foods and drinks that might interact with warfarin include:
Cranberries or cranberry juice
Grapefruit
Alcohol (including NyQuil and cough syrups)
Garlic
Black licorice
Foods that have a lot of Vitamin K.
Green leafy vegetables (Kale has the most)
Beets and Beet greens
Onions
Asparagus
Okra
Note to the caregiver
It will be okay if the patient uses any of the above as long as the caregiver ensures the use is consistent. The INR will pick up any changes and the dose will be adjusted, and conditions will stabilize. One-offs or minor occasional uses of any of the above won’t be a big deal. This is one case where doctors should be notified and consulted before any major change to the patient diet occurs.
Practical Hints For Caregivers
Contact sports may increase the risk of bleeding. No sword fights or full-contact football contests between the residents of your home, regardless of how entertaining that would be to watch. (just kidding around) Use an electric razor to shave.
Use a soft-bristled toothbrush and wax floss.
Fall proof the inside and outside of your home.
If bleeding occurs apply constant pressure to the wound. If this does not work seek further medical help.
Medical alert bracelets may be appropriate to use.
The different strengths of warfarin are colored differently to help not make mistakes in dosage.
Conclusion
Blood-thinners are an important but high-maintenance medication that can prevent serious illness and death. They require In-Home caregivers to:
Follow prescriber’s instructions faithfully
Monitor the patient for the signs and symptoms of bleeding
Help the resident to make the proper lifestyle choices
Help maintain stability in the variables that can affect blood-thinning therapy.
Like with many things in life, if the caregiver works at the above list hard it will become a matter of habit and become easy.
Credit Hours 2 - Approximate time required: 120 min.
Educational Goal
Differentiate between the flu and other common illnesses and how prevent and treat the flu.
Educational Objectives
Distinguish between viral influenza and other common diseases and conditions.
Teach about flu prevention
Provide Flu Prophylaxis alternatives
Explain how to properly treat of the flu.
Provide details about different Flu treatments
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.
Caregiver Focus on the Flu
With all the craziness on Covid capturing the public’s attention, it’s easy to forget that the regular flu is still around. It still makes people sick. It still puts people in the hospital. There is still a risk of death for the weak and infirm if they get the flu. Hey wait a minute, aren’t those the kind of patients you take care of in care homes? Maybe the flu is something you should focus on then. Just what is the flu anyway?
What is “The Flu”
The flu or influenza is one of those terms that have become fuzzy in the minds of the general public. Is it a cold that has gone bad? Is it the same as Pneumonia? What’s the deal with stomach flu? How do you treat cases of the flu? Are antibiotics involved? Who’s at the greatest risk for death? Being medical professionals, caregivers should know the answers to those questions. Having the right answers will help you take care of your people better.
According to the Bantam Medical Dictionary the flu is
“A highly contagious viral infection that affects the respiratory system.”
I want you to pay attention to the words “viral” and “respiratory”. We are not talking about a bacterial infection, just a virus. “Well, what’s the difference” you might be asking yourself. For the layman, it is very hard to tell the difference. The body has some of the same reactions or symptoms to both an infection caused by a bacterium or a virus. Namely runny nose, sneezing, cough, fever, sore throat, achiness, and being tired. Symptoms occur 1-4 days after exposure and usually resolve themselves in 7 to 10 days.
Virus
Bacteria
To make things easier for caregivers, it is important to note that bacterial infections are a lot less prevalent than viral influenza. So much so that it is safe to assume the flu was caused by a virus unless proven otherwise. On the other hand, to make things more complicated for caregivers it is possible to have both happen at the same time. No wonder the definition of the flu has gotten fuzzy. Most often the virus will start the infection. While the body is weakened, bacteria will start to grow out of control and make things worse.
Fortunately for caregivers, you have a doctor to fall back on. It’s their job to worry about such things. They have easy tests that they can run to determine if it’s a bacterium that is causing the symptoms or not. As far as you’re concerned your caregiving actions will be the same for both. The only difference in my opinion is when to start asking about getting an antibiotic prescription? Again, in my opinion, that is when symptoms are getting much worse or not resolving as expected.
Now you don’t want to be that caregiver who makes the doctor dispense a drug when one is not needed, “just in case”. In-home caregivers need to be better than that. There are a set of symptoms that you can watch for that will let you know when it’s time to call for an antibiotic.
Duke Heath website says,
Symptoms persist longer than the expected 10-14 days a virus tends to last
Fever is higher than one might typically expect from a virus
Fever gets worse a few days into the illness rather than improving
Okay, now that we have covered the bacteria/virus thing, lets clear up the fuzziness caused by other questions. Is the flu the same thing as pneumonia? The answer is yes and no, well sort of. Talk about being fuzzy. Pneumonia is a condition of inflammation and puss collection in the lungs that makes it hard to breathe. That should make it easier to understand. Simply put the Flu is an infection that can cause the condition of pneumonia. In other words, pneumonia is the flu that has gotten deadly serious. When your residents start having troubles breathing it’s time to start using the word pneumonia. Use the word as a motivator to get others to cooperate in getting advanced care for your sick resident.
Now what about the stomach flu. The stomach doesn’t seem to fit in the definition, right? Well, it turns out that the sometimes stomach upset is involved in the flu. I know, more fuzziness to clear up. Obviously, we are talking about caring for a patient who gets an upset stomach, diarrhea, and vomiting. In my research for this article, I found that viral influenza can often cause these problems in children. Also the swine flu is notorious for cause stomach problems. If stomach problems occur along with coughing, sneezing and fever it still might just be the flu. So caregivers, when you see the combinations symptoms you can start asking more informed questions of the doctor. I know it’s kind of vain, but you have to admit that it’s kind of a rush when you get a surprised look from the doctor when you ask an insightful question.
The last fuzziness to clear up is the infection a cold or the flu. Both are viral infections. The difference according to WebMD is severity of symptoms.
“Flu symptoms are usually more severe than cold symptoms and come on quickly. Symptoms of flu include sore throat, fever, headache, muscle aches and soreness, congestion, and cough. Swine flu in particular is also associated with vomiting and diarrhea.”
So In-home caregivers, it’s all about how much trouble is caused and how fast that trouble comes on. I guess how much “trouble” all depends on how infirm the client is? If you’ve got a strong as a bull client, who cares if it is a cold or the flu. They might complain a lot, but they’ll survive. But if you got a client that is weak as a new born lamb who cares if it is a cold or a virus. The doctor needs to get involved quickly. Practicality makes the fuzziness in definitions irrelevant.
I hope the flu fuzz is now gone. For the rest of this article, I will focus on viral infections of the respiratory system just like the medical dictionary said.
The Stats
According to data recently posted by the Center for Disease Control and Prevention (CDC), there have been up to 45 million cases of the flu, 810,000 hospitalizations, and 61,000 deaths annually. Statics of particular interest to In-Home Caregivers in the 2019-2020 flu season:
More than 52,000 hospitalizations occurred in children aged less than 18 years old.
86,000 hospitalizations among adults aged 18-49 years occurred.
Forty-three percent of hospitalizations occurred in older adults aged ≥65 years.
7,800 deaths (36% of all deaths) occurred among working-age adults (aged 18–64 years), an age group for which influenza vaccine coverage is often low
Approximately 62% of annual flu-related deaths occur among older adults.
Among the regular population of Americans, an outbreak of the flu is of moderate concern. It is an illness that resolves itself in less than 2 weeks. Hospitalization or death is a result of other issues in combination with influenza. The major risk factor for hospitalization and death seems to be from being infirm or having a chronic illness. Which is almost 100% of patients being taken care of by In-Home caregivers. I am confident in making that statement because if they weren’t infirm they would not be under your care. Even adults in mental health homes and youth in developmentally disabled homes can’t take care of themselves without you being there to keep them from getting sick.
In-Home Caregiving and the Flu
In-Home caregivers are uniquely suited to handle everything flu-related. You already know that you have the most power in influencing the people you take care of. The old hands in this industry know they can be relied upon to get things done at the right time and the right place if they know in advance what to do. After all, that is the reason why you’re taking the time to read this article, right? For those who are new to In-Home caregiving, you will see by the end of the article what an important part you can play in preventing and treating the flu in those you take care of. Let us lay the caregiving details out in the three Ps of influenza caregiving, -Prevention, Prophylaxis, and Proper treatment.
Prevention
A clean home and a healthy body are the best starts for flu prevention. That means cleaning and disinfecting frequently touched surfaces at home, (telephones, doorknobs, and various handles like bathroom faucets)
I recommend a disinfecting spray or cleaner (like Lysol or its equivalent) for surfaces. Alcohol wipes are another option. If it was me, I would stick with the soap and pull out the wipes if there is an active illness in the home. You can save money that way.
Get plenty of sleep, be physically active, manage your stress, drink plenty of fluids, and eat nutritious food. As far as personal hygiene, wash the virus off your hands often and protect the nose. The hand-to-nose path is a major route for viruses to travel. I don’t have as much confidence in just using alcohol wipes and hand sanitizing gels by themselves. I think it is better to use soap to remove the viruses off the skin than let them sit there hoping the alcohol will somehow kill off the virus.
Of course, good care homes are already doing all of the above as a matter of course. Great job, pat yourself on the back with a recently washed hand.
Unfortunately, a healthy person in a clean home can still get the flu. Up to 11% of the population can have influenza during the flu season. All of those sick people are sneezing and coughing, putting virus-filled droplets all over the place. Infected people will blow their noses then spread germs on any surface they touch. You come along and accidentally pick up a handful of viruses as you go shopping. You scratch your nose or rub your eyes and the infection spreads to you. You now carry the infection home, and you won’t show any outward signs of the flu for 1 to 4 days. All the while happily going about your business and spreading the virus to other surfaces as you go. Youth who go thru life clueless or thinking they are immortal are particularly talented at catching and spreading the influenza virus. They ignorantly travel through a virus-filled world and come home and give you a nice big hug. During flu season a giving family takes on a whole new meaning.
Clearly, In-Home caregivers need to do more to protect the ill and infirm in their care.
Prophylaxis
Prophylaxis is just a fancier way of saying prevention. Hang in there with me and you will see the difference from the previous paragraphs. I can sum it up in one word, Inoculation. If you hate needles, a shudder just went down your spine. Fortunately, in the case of preventing the flu, needles may not be involved. There are options for those who are afraid of getting poked by a syringe.
First, let’s talk about the process of inoculation. To inoculate means to introduce a substance into the body for the purpose of stimulating an immune response.
Now you don’t want to actually give the person the flu. So you alter the flu virus enough so you get the defense without causing the illness. It does not matter how the altered virus is introduced. As long as it gets into the bloodstream and the body defends itself by building up an immune response to the substance being introduced (antigen).
The quickest and easiest way to inoculate is to inject the antigen directly into the bloodstream via a needle. Fortunately for those who refused to be stuck with a needle the alternative is to introduce the antigen through the nasal passage blood vessels via a nasal spray (brand name FluMist Quadrivalent). There is a trade-off though. In order for the nasal inoculation process to work, they have to use LIVE but attenuated viruses. That means there is a slight chance that the person will actually get the flu. But I want to emphasize the word slight, meaning very, very small chance.
Because of this risk, Flumist is not recommended for children under two or people over 50, or anyone who has a weakened immune system. Oh, I almost forgot. They use eggs to produce some flu vaccines so people with egg allergies might have to use the nasal spray.
One more thing about inoculation. The flu virus has a nasty habit of mutating. Every year a new strain is discovered, and the inoculation process has to happen all over again. The bottom line for caregivers is to get your yearly flu inoculation. For yourself and the people, you take care of. It’s very easy to do, just go to the clinic or pharmacy to get flu pocked. They will handle all the prescription and payment issues. Depending upon circumstances, you might have to call ahead for the nasal spray and or go through some extra stuff to get the insurance to pay for it.
Just to be complete there is another prophylaxis method. That is stimulate or enhance the entire immune system through the use of Echinacea, mega-doses of vitamin C, or homeopathic medicine. Do these actually work? Well maybe, better than doing nothing I suppose. I personally have used homeopathic medicine for a cold but have little confidence in them preventing or treating the flu. Consult with your doctor before considering them for your residents.
Proper Treatment
Unfortunately, even with a clean home, a healthy immune system, and a flu shot, it is still possible to get the flu. Stubborn and ‘onery critter isn’t it. Or maybe the flu came before you got around to getting a flu shot. Regardless of the reason why, caregivers now have to deal with a sick person. Their efforts fall into three categories, disease treatment, symptom relief, and controlling the spread of the infection.
Disease Treatment
Disease treatment is stopping the infection and or reducing its severity. It may seem like an area where In-Home caregivers don’t have much say in, but you would be wrong. Caregivers can have a huge impact on disease treatment through the timing of therapy initiation and asking the prescriber the right questions. To truly appreciate your position, you have to understand something about viruses.
According to Scientific American
“For about 100 years, the scientific community has repeatedly changed its collective mind over what viruses are. First seen as poisons, then as life-forms, then biological chemicals, viruses today are thought of as being in a gray area between living and nonliving: they cannot replicate on their own but can do so in truly living cells and can also affect the behavior of their hosts profoundly… most evolutionary biologists hold that because viruses are not alive,” Source https://www.scientificamerican.com/article/are-viruses-alive-2004/
Viruses have a protein coat that surrounds some genes, basically, that’s all. They do not have the biological mechanics to replace themselves or grow. They have to rely on a “living” host cell to do so. Once a virus penetrates the cell, it hijacks the cell's mechanisms and replicates itself continually until the cell dies. The cell then bursts, releasing many more viruses to invade other cells. If they don’t enter a cell, they just sit there doing nothing until the immune system comes along and cleans things up.
If viruses aren’t technically alive the immune system cannot technically kill them. What the body does is send out antibodies that recognize the protein sequences in the outer coat. The antibody latches on to the virus and inhibits them from entering a cell and releasing its genes. They also signal other components of the immune system to come along and break up and destroy the virus. By the way that is what vaccines are, antibodies that recognize a certain virus. The important part for you to understand is that you have to catch the virus quickly before it enters a cell and hijacks the cell replication mechanisms. Only then will you stop the infection from spreading.
That is where In-Home caregivers can play such a significant role in disease treatment. They know the patient better than anyone else because they live with them. They will notice the signs and symptoms of a viral infection just as they start to show themselves. Then they get the patient to the clinic and tell the doctor the information he or she needs to know to initiate therapy.
Symptom recognition
In-Home caregivers do not have to know enough to make a diagnosis. They just have to know enough to suspect something is wrong that needs medical attention. The symptoms of a viral infection are:
fever or feeling feverish/chills
cough
sore throat
runny or stuffy nose
muscle or body aches
headaches
fatigue (tiredness)
some people may have vomiting and diarrhea, though this is more common in children than adults.
Sounds like a cold right? That is because a cold is a virus too. Flu viruses are much more virulent though, so symptoms come on quicker. Caregivers who are looking for signs of the flu should watch for a rapid onset of symptoms. It is also important to note that fever may or may not be among the first signs of the flu.
Instead, look for the tickle in the throat that will not go away after a sip of water and a cough. Also, look for the headache that quickly turns into body aches and chills. The chill part is important because that is a sign the body has recognized a threat and is rapidly contracting and relaxing muscles to produce heat to fight an infection.
If a fever starts to develop then, at first, help the body defenses by keeping the body warm. “feed a fever and starve a cold” Of course, if it gets quickly too hot that’s a different matter, and also a possible sign of the flu. Call your doctor if the temperature is 103 F (39.4 C) or higher regardless of how quickly it comes on.
A sudden unexplained fatigue or exhaustion is also an early sign that the body senses an infection coming on and is shifting its resources from everyday function to an immunity response.
But the biggest red flag for caregivers to watch for is if all of the above symptoms suddenly happen at the same time. Caregivers should then record all the specifics of their findings and call the doctor’s office. Include actual measurements when possible (days from onset of symptoms, temperature, and the like). Most importantly ask if these are possible signs of the flu coming on. That starts the doctor to quickly think in terms of the flu.
Doctor diagnosis
After the phone call, the doctor may issue a prescription right away if you have built up a reliable reputation of knowing what you are talking about. Most likely though he or she will want to examine the patient themselves. They will most likely turn you over to his office staff to make an appointment.
This is the second place where skilled In-Home caregivers can have a big impact. If the receptionist gives you an appointment anytime but Now then you might have to get kind of pushy. Do so politely by asking, “I think that we're talking about the flu and a quicker response might be needed. Are you sure you don’t have anything sooner? If the answer is no then you must acknowledge that the doctor has only so much time in a day and you have to seek quicker medical help. You can try a “first come first serve” medical clinic or the emergency room. The quick-service medical offices are popping up everywhere. It would be wise for a skilled caregiver to know where they are in their community in advance. It would also be wise to tell the doctor you used one after you have come back from the appointment at the stat clinic or ER.
Managing the Prescription
The third place where In-Home caregivers can have a huge impact is managing the drugs after the prescription has been written. It starts by deciding if the doctor is in the right ballpark. It is amazing to me that after all the information about developing bacteria resistance, antibiotics are still being prescribed for flu-like symptoms. In a recent study of 14987 patients who had upper respiratory infections between the years 2013-15, 41% were given antibiotics. The study determined that 84% of those given antibiotics had a viral infection.
So, after the prescriber hands you the prescription ask if it is an antibiotic. If it is or you recognize the drugs as an antibiotic beforehand it’s time to get pushy again by asking polite questions. I suggest, “Doctor I thought the symptoms were caused by a virus, isn’t there a test where you can use to rule out a viral infection. After all, if it is a virus time is important. By the way, the answer is yes, there are several virus antigens tests. If the doctor still insists on the antibiotic, then go with it and monitor the patient during therapy. If after 3 days the symptoms do not lessen or get worse, it’s time to call the doctor again. Bring up the virus question again or get a second medical opinion depending on how severe the symptoms are becoming. Use tact because you are going to have to work with this guy in the future.
If there is a viral infection diagnosis, there are 4 antiviral medications a prescriber can choose from.
Name
Route
Dosage
Oseltamivir (Tamiflu)
By Mouth
Once daily for 5 days
Peramivir (Rapivab)
IV infusion
One infusion
Zanamivir (Relenza)
Inhaler
Twice daily for 5 days
Baloxavir (Xofluza)
By Mouth
One single dose
This is the fourth place for In-Home caregiver input. You know your people better than the doctor does. If there is a problem with needles, like in small children, you might ask about Relenza. If there are problems with taking medications, like with mental health patients, then questions about Xofluza might be appropriate to ask.
There is a fifth place where skilled In-Home caregivers have to act, monitoring therapy. After two or three days if symptoms are not lessening or getting worse call the doctor. Depending on how severe the symptoms are, you might have to skip the doctor and go to the hospital. Especially in cases of difficulty breathing. Remember the pneumonia thing.
Even if the symptoms are lessening you still have to monitor signs of medication side effects. Fortunately in antivirals, the side effects are typically mild and will go away by themselves after therapy is done. Usually, all caregivers have to do is work with the patient to make them feel comfortable until therapy is over. Except for signs of an allergic response. If they happen call the prescriber right away. Watch for rash, swelling, itch and difficulty breathing. Take these signs seriously, for with each dose given there is a chance of ever greater allergic responses. Neuropsychiatric events (see * below) are also to be called into the doctor but are on the rare side.
Diarrhea, skin reactions, delirium, hallucinations, seizures, or unusual behavior *
Baloxavir (Xofluza)
Diarrhea, nausea, headache
Three final notes on medication management.
Taking antivirals with food can lessen nausea.
Xofluza should not be taken with anything that contains calcium, iron, or magnesium. They can stick to the drug and deactivate it. That included calcium-fortified foods, antacids, and vitamin supplements with mineral in it. Work with the doctor about which meds to change and make appropriate notes in the MARS about medication messed.
Taking an antiviral medication will mess with Flumist because it’s a Live but attenuated (not as virulent) virus. Steps will have to be taken to adjust inoculation therapy.
Symptoms
Relief
Symptom relief
It’s time for me to get my pharmacist hat on. I recommend the following for flu and cold symptom relief.
We have already covered, feed a fever-starve a cold,
Take with food for drug nausea. If you need a food suggestion, soda crackers are great for drug-induced nausea. Applesauce and Cream of Wheat or Cream of Rice are also easy on the stomach.
If diarrhea occurs, you probably don’t have to do anything beyond rehydration. The body is just trying to get rid of the nastiness quickly, so cooperate- don’t hinder, unless the doctor gives instructions to the contrary.
Rest is best for general malaise symptoms.
For pain, your regular PRN pain med will do, chiefly acetaminophen or NSAID. No aspirin for kids.
For coughing, I recommended anything with dextromethorphan. Look for the DM on the label. In my opinion, guaifenesin is not needed if you push the fluids and it makes the cough syrup taste bad. Also, you actually don’t want to stop the coughing if it is getting the cud out of the lungs.
I really don’t have any preferences for nasal sprays to help with breathing through the nose. Don’t forget nasal strips and Mentholated rubs. Mentholated rubs also feels good on sore muscles.
For sore throats, cough drops can do double duty here, but throat numbers are more effective, like Cepacol, Sucrets, or Chloraseptic. If the throat numbers don’t touch the throat soreness call the doctor and ask about a secondary strep throat infection.
Whatever you use, get PRN orders from the doctor so you don’t get in trouble. If you have preferences, write them down and send them to the doctor with a yes or no check box and a place for the doctor’s signature. Don’t forget the strength, quantity, and directions or you can’t use it at the pharmacy as a prescription. Just use the instructions off the package
Stopping the Spread
If taking care of one person with the flu sounds like a lot of work, can you imagine taking care of a whole household and yourself with the flu? What a caregiving nightmare. That is a real possible outcome if the flu penetrates your home's defenses. An infected person can spread the virus to others from day one of the infection. They remain contagious for up to 7 days. Those with a weakened immune system will take longer to get the virus under control so they may be contagious for up to 2 weeks. If someone brings the flu into your home, it’s time to kick caregiving into high gear.
Isolate the infected and make sure they are taking the right precautions to stop the spread.
Cover the mouth when coughing with a tissue or cough into their elbow.
Wash their hand often, especially after coughing, sneezing, or wiping the nose.
Super clean up after the sick, especially handles. (Time to pull out the alcohol wipes)
Have the rest of the household increase their hand washing. You can even issue those at high-risk bottles of saline nasal spray so they can keep their nasal passages cleaned out and virus-free.
You the caregiver should use universal precautions when taking care of the sick. Wear gloves and treat everything coming off the infected as if it was full of contagions. Use the nasal saline spray often yourself. Keep a can of disinfecting spray or alcohol wipes handy and use them often.
You can also get everyone inoculated but it may be too late for that to stop the spread of the flu. It takes a while for those inoculated to build up an immunity. What you can do is give those at high risk a prophylactic course of antiviral meds. In one study, 752 uninfected people took Xofluza and it reduced the risk of influenza by 86%. Discuss the possibilities with the doctor.
The Difference Between Covid and the Flu.
It’s time to talk about the elephant in the room. Covid is also a viral caused flu, just a nastier version of it. At first, it is going to look the same as regular flu except Covid can alter taste. It also has a longer incubation period before symptoms start to arise, between 2-14 days. All the regular flu precautions will work on Covid, but it will take a different flu shot. Antiviral meds will probably not be a good enough prophylaxis. Consult with the doctor to get their opinion on that. It is unclear how long a person will be contagious after they get Covid, we just don’t know yet.
Conclusion
See how important In-Home caregivers are in handling influenza. You are “Thee” expert on the 3 Ps of influenza caregiving. Prevention, Prophylaxis, and facilitating Proper treatment. You have true power. Now go out and protect your household and those you take care of with it.
As always Good Luck in your caregiving.
Mark Parkinson BsPharm
References:
Influenza Update: Pharmacist Focus on the Challenges of Early Identification and Timely Treatment. (Recorded Panel Discussion),Chair: Dennis Williams Pharm D.https://www.powerpak.com/course/content/120347
Flu Symptoms & Complications. Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases (NCIRD)Sept. 21, 2021https://www.cdc.gov/flu/symptoms/symptoms.htm
Credit Hours 1 - Approximate time required: 60 min.
Educational Goal
Teach caregiving management of salt consumption and sodium metabolism.
Educational Objectives
Teach about the physiology of sodium.
Provide a basic understanding about the pathophysiology of sodium.
Teach caregiving techniques on how to manage sodium consumption.
Tell how to reduce sodium consumption.
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.
Reducing Sodium
Salt, we love our salt. We flavor our dishes with it. We brine our meats in it, and we preserve our foods with it. We have a genuine appetite for salt. Look in any pantry and I bet you will find containers of table salt, popcorn salt, garlic salt, onion salt, pickling salt, seasoned salt, sea salt, and kosher salt. It should be no surprise to anyone that we consume a lot of salt but at what cost to our health?
The Chemistry of Sodium
Common table salt is a crystalline compound of sodium and chloride atoms. When chlorine and sodium atoms get together, chlorine takes an electron from the sodium, giving each a charge. Chlorine has a negative charge and sodium gets a positive charge. Like magnets, the opposite charges attract each other, and a uniform crystalline lattice forms.
Water is also a compound of different atoms. It has two hydrogens atoms and one oxygen atom. Oxygen does not take the electrons from the two hydrogens but shares them instead. Sharing electrons creates a stronger bond between the atoms. But doing so bends the shape of the molecule into a v shape. This v shape gives the water molecule a partial negative pole and a partial positive pole.
When you place a salt crystal in water the partial charge of the water molecule is strong enough to break up the crystal lattice but not strong enough to take any of the chlorine or sodium’s electrons. The result is you have Na+ and Cl- atoms called ions floating in the water.
So why all the chemistry mumbo jumbo. Our bodies are set up to take advantage of free-floating sodium molecules to perform many metabolic functions. The positive sodium ions attract free negatively charged electrons. As the electrons move around, an electric current is created. That is how a nerve signal is created. Also, the sodium ion charge attracts water. Wherever the sodium ion goes, water follows it around. If the body wants water to go someplace, it pumps the sodium ion there and the water naturally follows. Our muscles contract, we think and feel, pee, salivate, sweat, and a host of other functions all because of sodium.
Pathophysiology of Sodium
If there is too little sodium in the bloodstream the condition is called Hyponatremia. Too much sodium results in Hypernatremia. Cases can be mild, moderate, or severe, based on the concentration of sodium in the blood. The firing of nerves signals and the contraction of muscles both depend on the ionic charge of the sodium ion, Na+. In the most severe cases when the concentration of the ion is too much or too little, seizures, heart arrhythmias and death may occur.
Because water follows sodium, disorders of sodium are also disorders of water. If too little sodium is in the bloodstream, water will be drawn away into the cells where the salt concentrations are higher. The result is the cell swells and possibly bursts and dies. If there is too much sodium in the blood, then water flows into blood vessels increasing the body’s blood pressure. Chronically high blood pressure has its own set of problems and illnesses throughout the body, organs, and brain.
Fortunately, our bodies have ways to avoid severe cases of hypo and hypernatremia. Our bodies can control sodium’s impact through several homeostatic mechanisms that regulate sodium’s concentrations in the cells and bloodstream. Unless the change in sodium’s concentration is very quick, the body can adjust and avoid most of the severe cases of Hypo and Hypernatremia.
Caregiving and Severe Cases
For in-home caregivers’ severe cases of hypo and hypernatremia will be very rare. Acute severe cases would most likely occur in older adults who are
mentally and physically impaired,
do not eat or drink enough,
are sick with a high fever,
has vomiting,
has an infection that causes severe dehydration.
In-home caregivers should be on the lookout for symptoms in cases of severe vomiting, diarrhea, kidney or adrenal gland problems, and certain elderly populations. If the following signs occur call the doctor.
Hyponatremia
Hypernatremia
· Nausea and vomiting
· Headache
· Confusion
· Loss of energy, drowsiness and fatigue
· Restlessness and irritability
· Muscle weakness, spasms or cramps
· Seizures
· Excessive thirst
· Nausea and vomiting
· Loss of appetite
· Confusion
· Lethargy
· Muscle twitches
· Spasms
· Seizures
In-Home Caregiving and Salt
Hypo and hypernatremia are words that almost never come up in the In-home caregiving industry. What does come up all the time is reducing dietary salt as part of hypertension therapy. Harvard university summed it up in the following.
“In most people, the kidneys have trouble keeping up with excess sodium in the blood. As sodium accumulates, the body holds onto water to dilute the sodium. This increases both the amount of fluid surrounding cells and the volume of blood in the bloodstream. Increased blood volume means more work for the heart and more pressure on blood vessels. Over time, the extra work and pressure can stiffen blood vessels, leading to high blood pressure, heart attack, and stroke. It can also lead to heart failure. There is some evidence that too much salt can damage the heart, aorta, and kidneys without increasing blood pressure, and that it may be bad for bones, too.”
American adults eat an average of about 3,600 mg of sodium per day.
It has been recommended that we only need 2300 mg (1 teaspoon)
People with high blood pressure should have 1500 mg from all sources.
Reducing salt intake by 3 grams per day (1,200 mg of sodium) could cut the number of new cases of heart disease each year by as many as 120,000, stroke by 66,000, and heart attack by nearly 100,000. It could also prevent up to 92,000 deaths each year.”
It’s pretty clear Americans eat too much salt. Those who are infirm and or have high blood pressure need to consume less salt. So who is going to make that happen? The doctor, nurse, pharmacist- no it’s you. The responsibility to reduce salt intake rests on your shoulders, the In-home caregiver.
How to reduce sodium intake
Now we get to the real good stuff of the article. What In-Home caregivers can do about reducing salt consumption. Stats are good for scientific studies but are not that helpful for home use. Who has the time or the ability to measure how much salt is consumed in a home? We have to work with broad concepts that work on general outcomes for patients. It is the only practical way to proceed.
Start with lifestyle changes, not the saltshaker
We are used to viewing dietary salt through the lens of a saltshaker. That is not where you need to start. For an average person, 70% of the salt they consume comes from restaurants and prepackaged foods. That comes from the sandwich and fries from the burger joint, the convenience meal frozen pizza, the potato chip snack while watching TV, and the late-night burrito second supper. All of which are lifestyle choices the resident has made that you are now in control of. Salt reduction started to happen the minute you arrived on the scene. By controlling the menu and what is eaten for snacks you are accomplishing a significant salt reduction without even trying. Great Job In-Home caregiver. Keep up the good work of making regular scheduled homecooked meals and making wise snack choices (sodium reduction lifestyle choices).
Know where the Salt is hiding
Reducing the salt from a restaurant, convenience, and snack food is a good start. Now let’s work on the salt that is hiding in the foods you are cooking.
I went to my cupboard and found the salt content per serving in
Cream of Mushroom Soup 870mg
Hamburger Helper 530mg
Ramen noodles 780mg
The sodium amount was easy to find because it was written right in the Nutrition Facts panel on the package. To find which foods have the hidden salt all you have to do is read the label. The DV percentage column on the nutrition facts panel is a quick way to judge the salt content. Consider 5% DV or less of sodium per serving low, and 20% DV or more of sodium per serving high.
In general, you will find the most sodium in Prepared mixes, Packaged rice dishes, Soups, Canned foods, Frozen meals, and Packaged baked goods.
What can be done to reduce the hidden salt?
The answer can be had in one sentence, cook from scratch. “Ow”, I just felt all the mental daggers shot straight through my heart. I know it sounds like cooking from scratch is a lot of work, and you might think you don’t have the cooking skills for that kind of cooking. Let me tell you this, you are a better cook than you might think are. Also, it’s not that much extra work to cook from scratch. It’s just a matter of recipe modification, planning, and practice.
Take a slow cooker beef roast cooked in mushroom soup for instance. How much extra effort is it to replace the can of condensed soup with milk, mushrooms, and a little cream? Just that alone reduced the sodium per serving by 870mg. Skip the garlic salt, onion salt, and or seasoned salt. Instead, put in plain onion and garlic powder. Add a bit of lemon juice, pepper, paprika, chives, and a splash of reduced-sodium soy salt. Bingo, a delicious sodium-reduced beef roast. Work on the spice selection to match your tastes and it will taste better than the original high sodium recipe. All it took extra was just a few steps to the frig and less than 5 minutes of extra prep time. No big deal. You get the general principle, cooking from scratch allows you to cut out all the extra hidden salt even before reaching for a saltshaker.
Try these flavors to liven up your meals without salt.
Source: Flavor That Food, National Heart, Lung, and Blood Institute
A few extra reduced salt cooking tips
Substitute fresh or frozen products for canned products like fish or vegetables.
If you have to use canned, rinse the product in water before using
Make up your own sodium-reduced sauces and dishes in bulk. Then home can them or freeze them in easy-to-use meal size portions.
Buying products labeled "low-salt," or "no salt added
Avoid “cured” meats like ham or bacon, brined foods like pickles or sauerkraut, and sliced luncheon meats.
Cook rice, pasta, potatoes, and hot cereals without salt.
Premade grain products all contain at least some salt. Each slice of bread, biscuit or bagel, and or bowl of cereal when added all together is quite a lot of salt.
There are plenty of other sodium-reduced recipes and plans on the internet. The trick in using them is to stock up on the ingredients before you start cooking. Salt-free cooking starts in the grocery store.
A word on “reduced sodium” products
You might be tempted to take a cooking from scratch shortcut by using “reduced sodium” products. It’s an okay option but you need to know what they mean when you reduced sodium on a package label. According to the FDA on reduced-sodium food labels at the grocery store.
What It Says
What It Means
Salt/Sodium-Free
Less than 5 mg of sodium per serving
Very Low Sodium
35 mg of sodium or less per serving
Low Sodium
140 mg of sodium or less per serving
Reduced Sodium
At least 25% less sodium than the regular product
Light in Sodium or Lightly Salted
At least 50% less sodium than the regular product
No-Salt-Added or Unsalted
No salt is added during processing – but these products may not be salt/sodium-free unless stated
Salt from a saltshaker may not be as big a deal as you might have thought but it is an area that still needs to be worked on. The 10% of our salt consumption that comes from a shaker is used to fine-tune the flavor of the foods we eat. At least that is what we tell ourselves. In my years of cooking for a care home, I noticed that the saltshaker was used even before the food was tasted. Often saltshaker use was a habit more than a flavor selection.
I also noticed that the elderly used a lot of salt to compensate for not being able to taste foods like they use to. Instead of changing the recipe, they got into the habit of using the saltshaker instead.
As you know, patient habits are not set in stone. Over time habits and tastes can be changed. It’s all a matter of controlling inputs and being consistent in actions over time. Eventually, the sodium-reduced diet patient won’t even miss the salt. To help speed up the process I suggest that you make the table saltshaker disappear. Replace it with Salt substitute shakers. Mrs. Dash, NU-salt No-salt, Morton’s Salt substitute can all be found in the spice aisle. All but MRS Dash (which is a collection of dried herbs and spices) are made from potassium chloride instead of sodium chloride. Adding extra potassium to a diet is actually beneficial in many ways. It tastes different but you can get used to it quickly. They can go crazy with the shaker, and you won’t have to worry about it. Before using a lot of potassium chloride either in cooking or at the tablet you must know that extra potassium triggers extra stomach acid. Monitor for upset stomachs. The remedy is plain over-the-counter antacids. There are some medical considerations when using a lot of potassium. See my CE about potassium.
Conclusion
You can make this low-sodium thing work. After all, you are the lifestyle modifier expert. No one else in medical practice can accomplish the things that you can in your home. Your efforts will start at the grocery store as your look at labels and make food choices that steer you away from a high sodium diet and end at the shaker you use at the tablet. Making even a small reduction in sodium consumption can make difference for patients with high blood pressure. Studies have found that the DASH eating plan can lower blood pressure in as fast as 2 weeks. Is all the effort worth it- of course it is. Remember as you work towards a low sodium diet. Healthy patients are easy to take care of patients.
Most People Consume Too Much Salt. National Center for Chronic Disease Prevention and Health Promotiol, Division for Heart Disease and Stroke PreventionSep 14, 2021https://www.cdc.gov/salt/index.htm
Credit Hours 1 - Approximate time required: 60 min.
Educational Goal
Enable caregivers to properly fill out a Medication Administration Records Sheet.
Educational Objectives
Present the most common errors of filling out the MARS in a sarcastically humorous way.
Procedure:
Read the course materials. 2. Click on exam portal [Take Exam]. 3. If you have not done so yet fill in Register form (username must be the name you want on your CE certificate). 4. Log in 5. Take exam. 6. Click on [Show Results] when done and follow the instructions that appear. 7. A score of 70% or better is considered passing and a Certificate of Completion will be generated for your records.
Disclaimer
The information presented in this activity is not meant to serve as a guideline for patient management. All procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this article should not be used by care providers without evaluation of their patients’ Doctor. Some conditions and possible contraindications may be of concern. All applicable manufacturers’ product information should be reviewed before use. The author and publisher of this continuing education program have made all reasonable efforts to ensure that all information contained herein is accurate in accordance with the latest available scientific knowledge at the time of acceptance for publication. Nutritional products discussed are not intended for the diagnosis, treatment, cure, or prevention of any disease.
How to Mess Up a MARS in One Easy Lesson
There are those who just don’t learn a lesson until they suffer through the consequences of making a mistake. Following instructions, understanding the underlining principle or cooperation is just not their style. One would think that doing things the right way, in the beginning, would be easier but nooo. They feel it would be much easier to be lazy and put much more effort into correcting mistakes later on. Apparently, they just don’t feel successful until they mess up, get caught by government inspectors, and are forced to correct something later on.
I don’t personally think that would be good but evidently, a large portion of caregivers think this way when it comes to filling out a Medication Administration Records Sheet, or MARS for short. They must feel this way because they keep making the same mistakes on the MARS over and over again. Why else would they not learn from the past and change their behaviors?
So to make you feel successful, I want to help you fail and put much more effort into managing your medication duties than you have to. Because seemingly it feels good to fail an inspection of their MARS. So I present to you for your learning pleasure “How to mess up a MARS in one easy lesson”. I’m excited about this course because sarcasm is such a fun teaching method.
Responsibility
Now if you want to be embarrassed and fail miserably (and who doesn't want that bundle of joy) then there is no better way than to leave everything for someone else to do. Responsibility, who needs it anyway. It’s not like you have agreed to be in charge of keeping track of the resident’s medication. Just do as little as possible when it comes to the MARS and you’ll be fine. Of course, when mistakes happen (and they always do) you can always use the excuse that it was the pharmacy’s fault. Excuses make you feel better… until you realize that you are being held responsible for their errors. Not as much fun after that realization.
Periodic Chore
Being unsuccessful can be easy to achieve if you view the MARS as a periodic chore and not as a continual process that requires constant monitoring and action. If you don’t understand, try this experiment. Fill out the MARS once a day, once a week, once a month, and just before inspection. You will see that the longer you wait to fill out the MARS the more you have to lie when inspection times come. Nothing screams failure like being caught in a lie. A particular fast way of being caught is pre-filling out the MARS before you give out the meds.
Data
Do not use the MARS as a caregiver tool. You will also notice that the longer you wait to chart, the less effective the MARS becomes at gathering information. Information that helps you make your patients happier and healthier. Who needs to see long-term patterns, notice side effects, monitor therapy’s effectiveness? You’re just a highly paid babysitter anyway. No need to keep your residents well. It keeps you from getting bored if they are constantly unhealthy from the lack of proper medication management.
Initials
Hey, do you want to do something really fun? Do not put an up-t0-date initial key in the MARS. You know, that list that tells which initials belongs to which name. Stand back and watch the inspector try to go through the MARS. It’s hilarious to watch the frustration build. And if you want to kick it up a notch throw in some random initials that don’t correlate to anyone’s name but pertain to actions. For example, HO for a patient away at the hospital or RM for a patient refused medication.
Updates
A must-have skill that leads to failure is when a new physician order is obtained. Just cross out certain parts of the old MARS entry; (for example, strength or frequency), and write over it with the new instructions, instead of creating a new MARS entry. Nothing says I’m a medical amateur more than that particular piece of recordkeeping cleverness.
Missing Meds
Another must-have MARS skill is to leave off medications all together from the records. It’s way easier to just not list a medication. Who needs the hassle of keeping track of all those meds. The inspector never matches up the medication with the MARS anyway. Am I right or what?
OTC
Nothing says medical overreach quite like handing out OTC meds willy nilly. Look at you, acting just like a doctor. Deciding when to give out medication. Your momma would be proud. Never mind that you don’t have a license to prescribe medication. Who needs to follow doctor’s orders or follow package labeling when you have all that knowledge-based on your minutes and minutes of medical training? The doctor doesn’t need to know what going on. He can figure out that you changed his instructions all on his own. He is certainly smart enough to follow your lead in such matters.
Discontinued Medication
Do you want to really annoy the inspector and get revenge for being forced to do all that medical documentation work? Then keep initialing the MARS after a medication has been discontinued. Remember not to write down any notes on when the med was DCed. That will show ‘em. To kick the annoyance factor up a notch, just say “oops, I really haven’t been giving the medication, but I can’t remember exactly when I stopped giving it out.”
PRN
Speaking about annoying, PRN medications are the worst. They're just a whole list of record-keeping duties for each medication.
Each PRN has to have specific instructions. It’s not good enough to have PRN Pain. You have to have things like “as needed for hip pain every 4 to 6 hours, not exceed 3 doses per day”.
You have to fill out the time you gave out the med. So you can keep track of things like when the 4 to 6 hours are up.
You have to write down the outcome of the PRN therapy.
All that contacting the doctor for better instruction. All that extra writing. And they never give you enough space on the back of the MARS for proper note-taking. It’s such a hassle to put an extra piece of paper in the MARS. How’s a caregiver have enough time for the important things, like video games. Who cares if the PRN actually worked or if the frequency is changing or if the PRN is masking a serious developing condition and other such krap. To save time just give out the med on a regular basis and skip all that bothersome note-taking. That will lead to quick failure.
Halfway Thru Reality Check
Well we are halfway through the course. You are either loving this or hating every sarcastic joke. Or maybe it is becoming a bit uncomfortable. Am I getting a little too close to how you fill out your patient’s MARS? Am I starting to prick your conscience? The MARS is not a chore that is to be pared down to the easiest possible method of filling it out. If you do take the easiest possible route, you are missing all that wonderful information. Information that gives you power and control. You are an important part of the professional caregiving team, but only if you act like a professional. If you want to be seen as a babysitter and just want to be entertained, then by all means don’t try to understand the seriousness behind the jokes. Let’s get back to the sarcasm then. Now where was I? Oh yes, how to fail an inspection.
Missed or Refused Doses
If you are intent on failing an inspection, then leave the MARS blank with little or no explanation when the resident misses or refuses a dose. It will add a bit of mystery for the inspector to figure out. They will love that bit of intrigue you just added to their inspection.
Timing of Entry
There is a one-hour recordkeeping grace period before or after dispensing a medication, (wink, wink, nudge, nudge). Try using that as an excuse for not filling out the MARS on time and the inspector will have a giggle, giggle.
Same Dose Different Portions
It is okay to use the same MARS entry for different portioning of the drug if the overall dose doesn’t change. Example- two 5 mg tablets instead of one 10 mg tablet, or using powder instead of tablets. More winking and nudging…. and inspector giggling.
Mid-Month Changes
It is such a hassle when doctors make changes mid-month. Don’t they know all the extra work that entails? They are doing that just to spite you, yah know.
With every change you gotta;
Notify the pharmacy
Discontinue the old medication order, if there is one, and add an explanation note
Create a new MARS entry. Probably have to handwrite it in, while the pharmacy makes a new MARS.
Then you have to check the one the pharmacy generates to see if they got it right. Of course they won’t get it right. So you gotta call them up and do it all over again.
All that extra recordkeeping will require way too much time away from your favorite TV show. Just ignore changes until the new month rolls around. That’s an effective time-saving way to fail an inspection.
Timing of Doses
Speaking of saving time, Put AM or PM instead of the actual time you gave the dose. When the dose is given weekly or monthly do not mark out the days they are not supposed to give the medication. Who needs to have all that recordkeeping accuracy?
Allergies
If you are tired of failing the MARS inspections in the same old ways, try messing up the allergies for a change of pace. Writing down that the resident has no known allergies but is taking an allergy medication is a particularly effective technique for failing an inspection. Don’t forget to forget food and pet allergies and too.
Legibility
For more variety in failing, write all your initials, signatures, and notes so quickly and sloppily that nobody can read them. Include one initial instead of two. The initial of your last name will be just fine. It’s not like others in your family have the same last initial. Their sloppy handwriting will be different from your sloppy handwriting anyway.
Incomplete Records
There is no better method to avoid work while generating more work later on than having incomplete instructions. You know, unnecessary things like
Do not exceed …
Take with food
Inhale by mouth
As needed for …..
Strength, time, route of administration
It is so satisfying to avoid having to write all those pesky details in the MARS. Too bad that you’ll have to start completely over and do it all again the right way after you’re halfway through the month. Makes perfectly good sense doesn’t it.
Conclusion
Well I hope you enjoy the sarcastic comedy. Even though we had some fun I am as serious as any county inspector about doing the MARS right way. Keeping track of all the medications and data in real-time (not a week down the road) is so important. You are the frontlines of the care profession. The guy or gal in the medical trenches. You see the changes before anyone else. You can know your clients better than anyone else. But you got to utilize the tools at hand better than what we have been doing in the past.
Keeping up on the MARS will also keep you out of trouble with the state inspectors. Want to keep the state off your back? Then have a perfect MARS. It sends all the right messages to the inspector, doctors, pharmacy, and any other medical professional.
Having accurate, useable data will also give you power that you can use as the patient’s advocate. You can take the MARS to the doctor and say, “We have a problem. See this pattern right here in the MARS, do something about it- Now.”
Well that is enough preaching for now. This CE was supposed to be fun. I hope you liked it and can use the information it contained to be better at filling out the MARS. And NO, I don’t really want you to fail and have to do everything over again. Why would any caregiver want to do that, repeat that failing multiple times? It just doesn’t make any sense.
As always Good Luck in your Caregiving Efforts.
Mark Parkinson BsPharm
Warning: An unusual CE requires an unusual quiz. You have to prove you read the material by passing the test, so have patients with the weird questions.


 Lifting and Transferring Equipment
Lifting and Transferring Equipment New patient transfer equipment that is well within the reach of most care home budgets includes:
New patient transfer equipment that is well within the reach of most care home budgets includes: than $5.00 a piece used, they are being replaced by gait belts with a superior design. The new designs are two to three times as wide, made of easy-to-clean synthetic materials, a quick-release plastic clasp, and multiple soft handle loops sticking out. They are easier to use and clean than the older version. They cost a bit more, but new units cost less than $40.00.
than $5.00 a piece used, they are being replaced by gait belts with a superior design. The new designs are two to three times as wide, made of easy-to-clean synthetic materials, a quick-release plastic clasp, and multiple soft handle loops sticking out. They are easier to use and clean than the older version. They cost a bit more, but new units cost less than $40.00. Transfer Boards
Transfer Boards





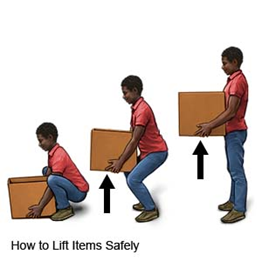


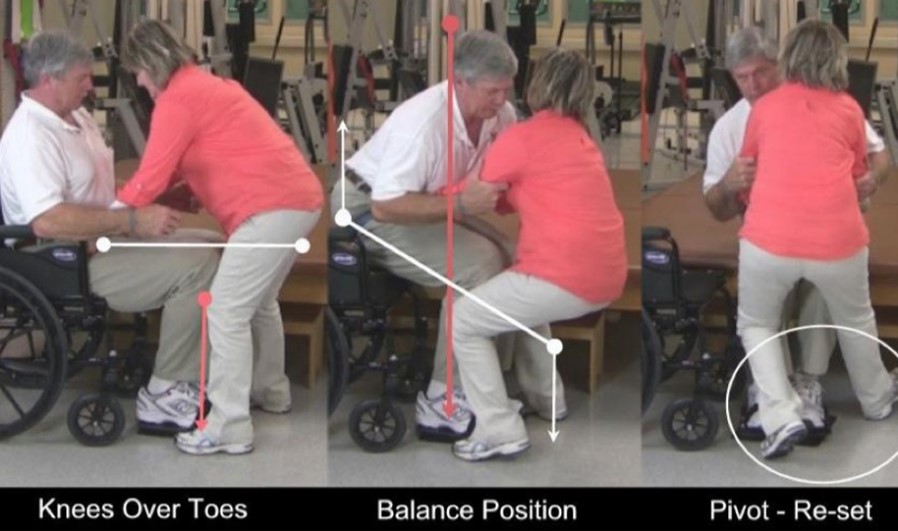



 Stages from the floor
Stages from the floor

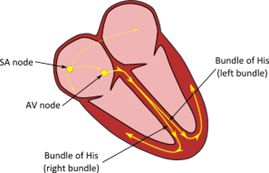



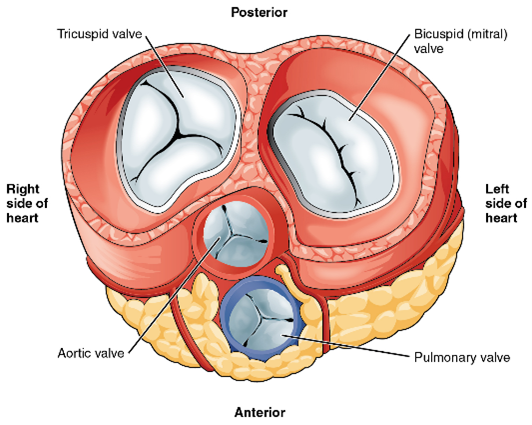
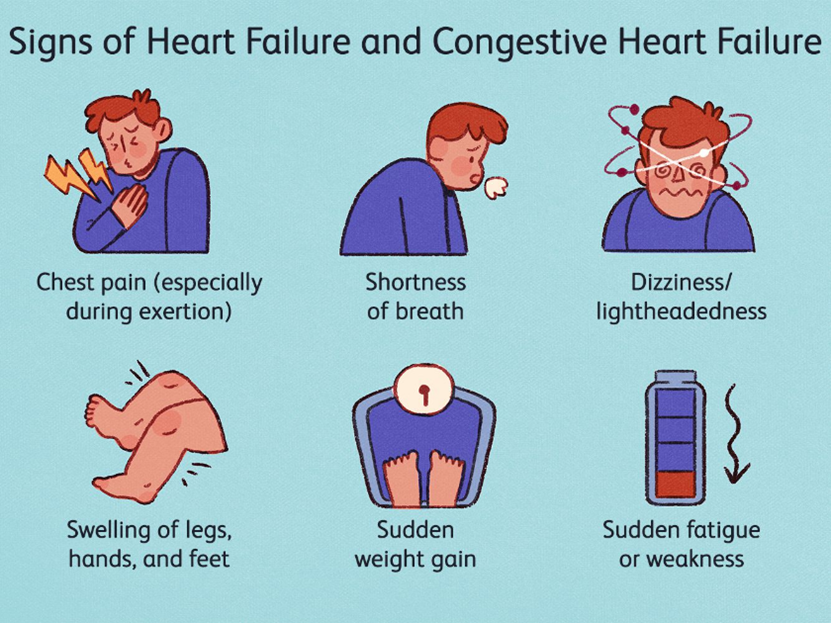











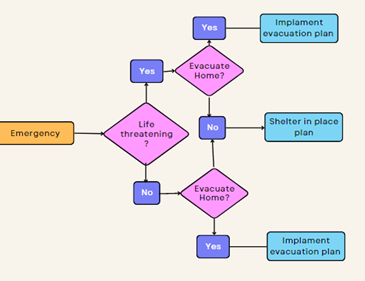




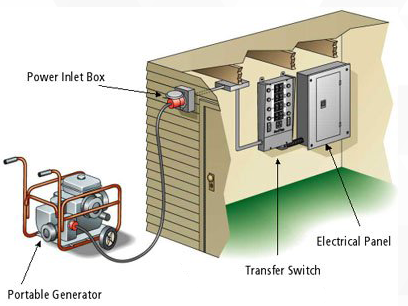


















 One trick I heard of is giving a baby doll to take care of. The doll can become real in a sense and have a great calming effect. Some memory care units even have baby stations.
One trick I heard of is giving a baby doll to take care of. The doll can become real in a sense and have a great calming effect. Some memory care units even have baby stations.








 When I was operating my own adult foster care homes there was one medication that constantly resulted in uncomfortable questions for county health officials, Warfarin (Coumadin). Warfarin is comely known as a blood thinner, we called it the bruiser medication. Blood thinners reduce the chances of dangerous internal blood clots that can cause a lot of damage. They also make it easier for minor cuts and abrasions to bleed profusely on the inside and outside. If an elderly resident bumped into the door a little too hard, a rather large bruise would inevitably form. It made it look like we took a bat and beat up the resident. Not a good look for a care home. It always resulted in abuse questions. Blood thinners are a high maintenance drug class that requires the In-Home caregiver to manage the patient and medication- carefully.
When I was operating my own adult foster care homes there was one medication that constantly resulted in uncomfortable questions for county health officials, Warfarin (Coumadin). Warfarin is comely known as a blood thinner, we called it the bruiser medication. Blood thinners reduce the chances of dangerous internal blood clots that can cause a lot of damage. They also make it easier for minor cuts and abrasions to bleed profusely on the inside and outside. If an elderly resident bumped into the door a little too hard, a rather large bruise would inevitably form. It made it look like we took a bat and beat up the resident. Not a good look for a care home. It always resulted in abuse questions. Blood thinners are a high maintenance drug class that requires the In-Home caregiver to manage the patient and medication- carefully. 






 Virus
Virus Bacteria
Bacteria
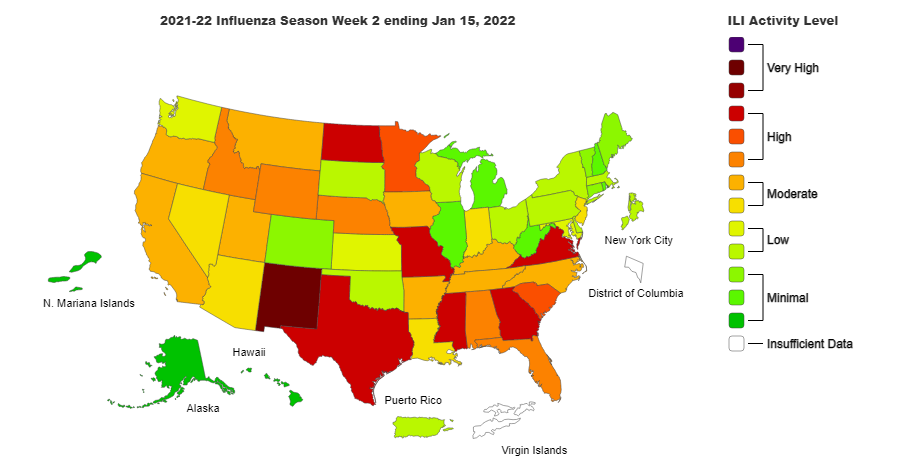
 Viruses have a protein coat that surrounds some genes, basically, that’s all. They do not have the biological mechanics to replace themselves or grow. They have to rely on a “living” host cell to do so. Once a virus penetrates the cell, it hijacks the cell's mechanisms and replicates itself continually until the cell dies. The cell then bursts, releasing many more viruses to invade other cells. If they don’t enter a cell, they just sit there doing nothing until the immune system comes along and cleans things up.
Viruses have a protein coat that surrounds some genes, basically, that’s all. They do not have the biological mechanics to replace themselves or grow. They have to rely on a “living” host cell to do so. Once a virus penetrates the cell, it hijacks the cell's mechanisms and replicates itself continually until the cell dies. The cell then bursts, releasing many more viruses to invade other cells. If they don’t enter a cell, they just sit there doing nothing until the immune system comes along and cleans things up.  If viruses aren’t technically alive the immune system cannot technically kill them. What the body does is send out antibodies that recognize the protein sequences in the outer coat. The antibody latches on to the virus and inhibits them from entering a cell and releasing its genes. They also signal other components of the immune system to come along and break up and destroy the virus. By the way that is what vaccines are, antibodies that recognize a certain virus. The important part for you to understand is that you have to catch the virus quickly before it enters a cell and hijacks the cell replication mechanisms. Only then will you stop the infection from spreading.
If viruses aren’t technically alive the immune system cannot technically kill them. What the body does is send out antibodies that recognize the protein sequences in the outer coat. The antibody latches on to the virus and inhibits them from entering a cell and releasing its genes. They also signal other components of the immune system to come along and break up and destroy the virus. By the way that is what vaccines are, antibodies that recognize a certain virus. The important part for you to understand is that you have to catch the virus quickly before it enters a cell and hijacks the cell replication mechanisms. Only then will you stop the infection from spreading. 

 So, after the prescriber hands you the prescription ask if it is an antibiotic. If it is or you recognize the drugs as an antibiotic beforehand it’s time to get pushy again by asking polite questions. I suggest, “Doctor I thought the symptoms were caused by a virus, isn’t there a test where you can use to rule out a viral infection. After all, if it is a virus time is important. By the way, the answer is yes, there are several virus antigens tests. If the doctor still insists on the antibiotic, then go with it and monitor the patient during therapy. If after 3 days the symptoms do not lessen or get worse, it’s time to call the doctor again. Bring up the virus question again or get a second medical opinion depending on how severe the symptoms are becoming. Use tact because you are going to have to work with this guy in the future.
So, after the prescriber hands you the prescription ask if it is an antibiotic. If it is or you recognize the drugs as an antibiotic beforehand it’s time to get pushy again by asking polite questions. I suggest, “Doctor I thought the symptoms were caused by a virus, isn’t there a test where you can use to rule out a viral infection. After all, if it is a virus time is important. By the way, the answer is yes, there are several virus antigens tests. If the doctor still insists on the antibiotic, then go with it and monitor the patient during therapy. If after 3 days the symptoms do not lessen or get worse, it’s time to call the doctor again. Bring up the virus question again or get a second medical opinion depending on how severe the symptoms are becoming. Use tact because you are going to have to work with this guy in the future.  There is a fifth place where skilled In-Home caregivers have to act, monitoring therapy. After two or three days if symptoms are not lessening or getting worse call the doctor. Depending on how severe the symptoms are, you might have to skip the doctor and go to the hospital. Especially in cases of difficulty breathing. Remember the pneumonia thing.
There is a fifth place where skilled In-Home caregivers have to act, monitoring therapy. After two or three days if symptoms are not lessening or getting worse call the doctor. Depending on how severe the symptoms are, you might have to skip the doctor and go to the hospital. Especially in cases of difficulty breathing. Remember the pneumonia thing.
/__opt__aboutcom__coeus__resources__content_migration__serious_eats__seriouseats.com__2019__08__20190819-salt-guide-vicky-wasik16--1500x1125-af406f896440419d8abdead0027a1d04.jpg)
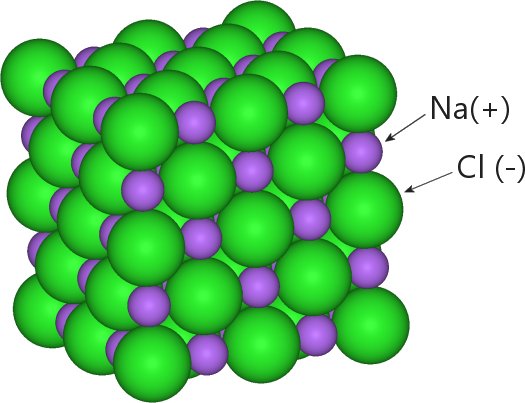 Common table salt is a crystalline compound of sodium and chloride atoms. When chlorine and sodium atoms get together, chlorine takes an electron from the sodium, giving each a charge. Chlorine has a negative charge and sodium gets a positive charge. Like magnets, the opposite charges attract each other, and a uniform crystalline lattice forms.
Common table salt is a crystalline compound of sodium and chloride atoms. When chlorine and sodium atoms get together, chlorine takes an electron from the sodium, giving each a charge. Chlorine has a negative charge and sodium gets a positive charge. Like magnets, the opposite charges attract each other, and a uniform crystalline lattice forms. 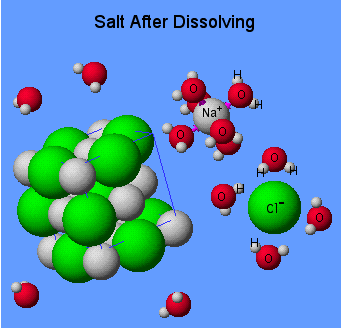

 What can be done to reduce the hidden salt?
What can be done to reduce the hidden salt? Salt from a saltshaker may not be as big a deal as you might have thought but it is an area that still needs to be worked on. The 10% of our salt consumption that comes from a shaker is used to fine-tune the flavor of the foods we eat. At least that is what we tell ourselves. In my years of cooking for a care home, I noticed that the saltshaker was used even before the food was tasted. Often saltshaker use was a habit more than a flavor selection.
Salt from a saltshaker may not be as big a deal as you might have thought but it is an area that still needs to be worked on. The 10% of our salt consumption that comes from a shaker is used to fine-tune the flavor of the foods we eat. At least that is what we tell ourselves. In my years of cooking for a care home, I noticed that the saltshaker was used even before the food was tasted. Often saltshaker use was a habit more than a flavor selection.  There are those who just don’t learn a lesson until they suffer through the consequences of making a mistake. Following instructions, understanding the underlining principle or cooperation is just not their style. One would think that doing things the right way, in the beginning, would be easier but nooo. They feel it would be much easier to be lazy and put much more effort into correcting mistakes later on. Apparently, they just don’t feel successful until they mess up, get caught by government inspectors, and are forced to correct something later on.
There are those who just don’t learn a lesson until they suffer through the consequences of making a mistake. Following instructions, understanding the underlining principle or cooperation is just not their style. One would think that doing things the right way, in the beginning, would be easier but nooo. They feel it would be much easier to be lazy and put much more effort into correcting mistakes later on. Apparently, they just don’t feel successful until they mess up, get caught by government inspectors, and are forced to correct something later on. Initials
Initials



